Antipyretics for children are prescribed by a pediatrician. But there are emergency situations for fever when the child needs to be given medicine immediately. Then the parents take responsibility and use antipyretic drugs. What is allowed to be given to infants? How can you lower the temperature in older children? What medications are the safest?
The liver (hepar) is the largest gland (its mass is 1500 g), combining several important functions. In the embryonic period, the liver is disproportionately large and performs the function of hematopoiesis. After birth this function fades away. First of all, the liver performs an antitoxic function, which consists in neutralizing phenol, indole and other products of decay in the large intestine, which are absorbed into the blood. Converts ammonia as a product of intermediate protein metabolism into less toxic urea. Urea is highly soluble in water and is excreted from the body in urine. As a digestive gland, the liver produces bile, which passes into the intestines to aid digestion. An important function of the liver is participation in protein metabolism. Amino acids, entering the blood through the intestinal wall, are partially converted into proteins, and many reach the liver. The liver is the only organ capable of converting lipoprotein cholesterol into bile acids. Liver cells synthesize albumin, globulin and prothrombin, which are carried throughout the body through the blood and lymph flow. It is no coincidence that 60-70% of all the body’s lymph with a high protein content is formed in the liver. Liver cells synthesize phospholipids that are part of the nervous tissue. The liver is where glucose is converted into glycogen. The reticuloendothelial system of the liver is actively involved in the phagocytosis of dead red blood cells and other cells, as well as microorganisms. Thanks to a well-developed vascular system and contraction of the sphincters of the hepatic veins, the liver is a blood depot in which intensive metabolism occurs.
262. Liver and its ligaments from the side of the diaphragmatic surface (according to R. D. Sinelnikov).
1 - lig. triangulare; 2 - lobus sinister; 3 - lig. falciforme hepatis; 4 - lig. teres; 5 - margo inferior; 6 - vesica fellea; 7 - lobus dexter; 8 - lig. triangulare; 9 - lig. coronarium hepatis.

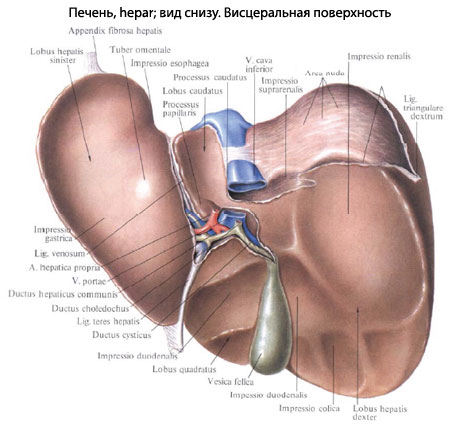
263. Liver from the visceral surface (according to R. D. Sinelnikov).
1 - lobus quadratus; 2 - impressio duodenalis; 3-lig. teres hepatis; 4 - ductus cysticus; 5 - ductus choledochus; 6 - ductus hepaticus communis; 7-v. portae; 8-v. hepatica propria; 9 - lobus sinister; 10 - impressio gastrica; 11 - impressio esophagea; 12 - lobus caudatus; 13 - v. cava inferior; 14 - impressio suprarenalis: 15 - impressio renalis; 16-lig. triangulare dextrum; 17 - lobus dexter; 18 - impressio colica; 19 - vesica fellea.
The liver has a wedge-shaped shape with two surfaces: facies diaphragmatica et visceralis, separated from each other by a sharp anterior edge and a blunt posterior one. The diaphragmatic surface is convex and, naturally, faces the diaphragm (Fig. 262). The visceral surface is somewhat concave, with grooves and imprints of organs (Fig. 263). In the center on the visceral surface of the liver in the horizontal plane there is a transverse groove (sulcus transversus) 3-5 cm long, representing the portal of the liver. The hepatic artery, portal vein, bile ducts and lymphatic vessels. The vessels are accompanied by nerve plexuses. On the right, the transverse groove connects with the longitudinal groove (sulcus longitudinalis dexter). In front of the latter lies gallbladder, and in the back - the inferior vena cava. On the left, the transverse groove also connects with the longitudinal groove (sulcus longitudinalis sinister), where the round ligament of the liver lies in the anterior part, and the remainder of the venous duct, which connects the portal and inferior vena cava during intrauterine development, in the posterior part.
There are four unequal lobes in the liver: the right (lobus dexter) - the largest, the left (lobus sinister), the square (lobus quadratus) and the caudate (lobus caudatus). The right lobe is located to the right of the right longitudinal sulcus, the left lobe is located to the left of the left longitudinal sulcus. In front of the transverse groove and on the sides, bounded by longitudinal grooves, there is a quadrate lobe, and behind the caudate lobe. On the diaphragmatic surface you can see the border of only the right and left lobes, separated from each other by the falciform ligament. The liver is covered by peritoneum on almost all sides, with the exception of the transverse groove and the posterior edge. The peritoneum has a thickness of 30-70 microns; interlobular layers extend from its connective tissue layer into the parenchyma. Therefore, mechanically, the liver is a very delicate organ and is easily destroyed.
At the junction of the peritoneum from the diaphragm to the liver and from the liver to the internal organs, ligaments are formed that help hold the liver in a certain position. Intra-abdominal pressure plays a role in liver fixation.
Ligaments. The falciform ligament (lig. falciforme) is located in the direction from front to back. It consists of two layers of peritoneum that pass from the diaphragm to the liver. At an angle of 90° it connects to the coronary ligament, and anteriorly to the round ligament.
The coronary ligament (lig. coronarium) is complex (Fig. 262). On the left lobe it consists of two sheets; on the right lobe, starting from the level of the inferior vena cava, the sheets of peritoneum diverge and between them a section of the liver of the posterior edge, not covered by peritoneum, is exposed. Ligaments hold the liver on the posterior abdominal wall and do not prevent the anterior edge from moving when the position of the internal organs changes and the respiratory displacement of the diaphragm.
The round ligament (lig. teres hepatis) begins in the left longitudinal groove and ends on the anterior abdominal wall near the navel. It represents a reduced umbilical vein, through which arterial blood flows in the fetus. This ligament secures the liver to the anterior abdominal wall.
The left triangular ligament (lig. triangulare sinistrum) is located between the diaphragm and the left lobe of the liver in front of the abdominal esophagus. On the left it ends with a free edge, and on the right it continues into the coronary ligament.
The right triangular ligament (lig. triangulare dextrum) connects the diaphragm to the right lobe of the liver, consists of two layers of peritoneum and represents the terminal part of the coronary ligament.
From the liver to internal organs more ligaments come off, described in the relevant sections: ligg. hepatogastricum, hepatorenale, hepatocolicum, hepatoduodenale. The last ligament contains the hepatic artery, portal vein, common bile, cystic and hepatic ducts, lymphatic vessels and nodes, and nerves.
The internal structure of the liver is represented by liver cells, which are united into hepatic beams, and the beams are connected into lobules; The lobules form 8 segments, which are connected into 4 lobes.
The parenchyma ensures the movement of blood from the portal vein, which is under low pressure (10-15 mm Hg), into the inferior vena cava. Consequently, the structure of the liver is determined by the architecture of the blood vessels.
The gate of the liver includes the portal vein (v. portae), which carries venous blood from all unpaired organs abdominal cavity, from the stomach, spleen, small and large intestines. In the liver, at a depth of 1 -1.5 cm, the portal vein is divided into right and left branches, which give rise to 8 large segmental branches (Fig. 264) and, accordingly, 8 segments are distinguished (Fig. 265). Segmental veins are divided into interlobular and septal, which break up into wide capillaries (sinusoids) located in the thickness of the lobule (Fig. 266).

264. Branching of the portal vein (purple) and hepatic vein (blue) in the liver (according to Yu. M. Dederer et al.).

265. Shape of the eight segments of the liver (according to Couinaud). A - view from the diaphragmatic surface; B - view from the visceral surface.

266. Sinusoids of the liver lobules.
1 - shape of sinusoids on the periphery of the lobule; 2 - sinusoids in the central sections of the lobule.

267. Histological structure of the liver lobule. 1 - interlobular branch of the portal vein; 2 - interlobular artery; 3 - interlobular bile duct; 4 - central vein; 5 - blood sinusoids (capillaries) and hepatic beams.
Along with the portal vein passes the hepatic artery, the branches of which accompany the branches of the portal vein. The exception is those branches of the hepatic artery that supply blood to the peritoneum, bile ducts, walls of the portal vein, hepatic artery and vein. The entire liver parenchyma is divided into lobules, which represent formations for more optimal transfer of blood from the portal vein and hepatic artery to the hepatic veins, and then to the inferior vena cava. There are layers between the lobules connective tissue(Fig. 267). At the junction of 2 - 3 lobules, an interlobular artery, vein and bile duct pass, accompanied by lymphatic capillaries. Liver cells are arranged in two-layer beams, oriented radially to the center of the lobule. Between the beams there are blood capillaries, which collect in the central vein of the lobule and form the beginning of the hepatic veins. Bile capillaries begin between two rows of liver cells. Thus, the liver cells, on the one hand, are in contact with the endothelium of the sinusoids and reticular cells through which mixed blood flows, and on the other, with the bile capillaries. The wall of the sinusoids and the liver cells are braided with reticular fibers, creating a framework for the liver tissue. Sinusoids from the interlobular vein penetrate into adjacent lobules. These sections of the lobules, supplied with blood from the interlobular vein, are combined into a functional unit - the acinus, where the interlobular vein occupies a central place (Fig. 268). The acinus is clearly revealed in pathology, since the zone of necrosis of liver cells and new connective tissue are formed around the acinus, separating the hemodynamic unit - the lobule.

268. Schematic representation of the lobules and acini of the liver.
1 - interlobular branch of the portal vein; 2 - interlobular artery; 3 - interlobular bile duct; 4 - slice; 5 - acini; 6 - central veins of the lobules.
Topography. The right lobe of the liver lies in the right hypochondrium and does not protrude from under the costal arch. The anterior edge of the left lobe crosses the costal arch on the right at the level of the VIII rib. From the end of this rib, the lower edge of the right lobe, and then the left, crosses the epigastric region in the direction of the bony part of the anterior end of the VI rib and ends along the midclavicular line. In the epigastric region, the surface of the liver is in contact with the parietal peritoneum of the anterior abdominal wall. The upper border on the right along the midclavicular line corresponds to the fifth rib, on the left, slightly lower, to the fifth-sixth intercostal space. This position is due to the larger right lobe and the smaller left lobe, which is under pressure from the heaviness of the heart.
The liver is in contact with many organs of the abdominal cavity. On the diaphragmatic surface, which is in contact with the diaphragm, there is a cardiac impression (impressio cardiaca). On the posterior surface there is a deep groove for the inferior vena cava (sulcus v. cavae), and to the left there is a less pronounced vertebral depression. A large area of the liver is in contact with other organs on the visceral surface. On the visceral surface of the right lobe there is an adrenal depression (impressio suprarenalis), a mild esophageal depression (impressio esophagea), a renal depression (impressio renalis), a gastric depression (impressio gastrica), there is an imprint of the upper bend of the duodenum (impressio duodenalis), the most pronounced depression of the right colon intestines (impressio colica). The left lobe of the liver is in contact with the caudal region and the lesser curvature of the stomach.
The liver of a newborn is relatively larger (40%) than that of an adult. Its absolute weight is 150 g, after a year - 250 g, in an adult - 1500 g. In children, the left lobe of the liver is equal to the right, and then it lags behind the right lobe in growth. The lower edge of the liver comes out from under the costal arch. On the visceral surface of the liver in a deep fossa (fossa vesicae felleae) lies the gallbladder.
22179 0
Anatomy of the liver
The liver has a wedge shape and rounded edges. The base of the wedge is its right half, which gradually decreases towards the left lobe. In adults, the length of the liver is on average 25-30 cm, width - 12-20 cm, height - 9-14 cm. The weight of the liver in an adult is on average 1500 g. The shape and weight of the liver depend on age, body structure and series other factors. The shape and size of the liver are significantly affected by the pathological process occurring in it. With cirrhosis, the weight of the liver can increase 3-4 times. The liver has two surfaces: visceral and diaphragmatic. The diaphragmatic surface has a spherical shape corresponding to the dome of the diaphragm. The visceral surface of the liver is uneven. It is intersected by two longitudinal grooves and one transverse, which, when connected, form the letter “H”. On the lower surface of the liver there are traces of adjacent organs. The transverse groove corresponds to the porta hepatis. Through this groove, vessels and nerves enter the organ, and bile ducts and lymphatic vessels emerge from it. In the middle part of the right longitudinal (sagittal) groove is the gallbladder, and in the posterior part is the inferior vena cava (IVC). The left longitudinal groove separates the left lobe from the right. In the posterior part of this groove there is a residual part of the ductus venosus (duct of Aranti), which in intrauterine life connects the PV with the IVC. In the anterior part of the left longitudinal groove is the round ligament of the liver, through which the umbilical vein passes.Liver lobes
According to Quineux's classification, the liver is divided by the transverse and falciform ligaments into two main lobes - left and right. The liver lobes differ in size from each other. In addition to the right and left, there are quadrate and caudate lobes. The quadrate lobe is located between the posterior or longitudinal grooves. In rare cases, there are additional lobes (the result of liver ectopia), which are located under the left dome of the diaphragm, in the retro-peritoneal space, under the duodenum, etc.The liver is divided into autonomous areas, sectors and segments, which are separated by grooves (depressions). There are five sectors - right, left, lateral, paramedian and caudate and 8 segments - from I to VIII.
Each lobe is divided into two sectors and 4 segments: 1-4 segments make up the left lobe, and 5-8 - the right. This division of the liver is based on the intrahepatic branching of the PV, which determines its architectonics. The segments, radially located around the porta hepatis, form sectors (Figure 1).
Figure 1. Anatomical relationships of the veins of the portal and caval systems and the segmental structure of the liver according to Quino-Shalkin
Each of these segments has two vascular - Glissonian - legs, consisting of branches of the hepatic artery, hepatic artery and CBD, and caval legs, which include branches of the hepatic veins (HV).
Structural classification of the liver is important for topical diagnosis of surgical intervention and correct determination of the location and boundaries of pathological formations and foci. The entire surface of the liver is covered with a thin connective tissue (Glissonian) capsule, which thickens in the area of the portal of the liver and is called the portal plate.
The study of the structure of the liver made it possible to determine the extent of pathological processes and the expected extent of liver resection, as well as to pre-identify and ligate the vessels of the removed part of the liver under conditions of minimal bleeding and, finally, to remove large areas of the liver, without the risk of impairing blood circulation and the outflow of bile from other parts.
The liver has a dual circulatory system. The outflow of blood from the liver is carried out by the PV system, which flows into the IVC.
In the area of the portal of the liver, on its visceral surface between the longitudinal and transverse grooves, large vessels and bile ducts are located superficially, outside the liver parenchyma.
Ligaments of the liver
The peritoneal cover of the liver, passing onto the diaphragm, abdominal wall and adjacent organs, forms its ligamentous apparatus, which includes the falciform, round, coronary, hepatophrenic, hepatorenal, hepatoduodenal and triangular ligaments (Figure 2).
Figure 2. Ligaments of the liver (anterior surface of the liver):
1 - lig. triangulare sinistrum: 2 - left lobe of the liver: 3 - lig. faidform; 4 - lig. teres hep-atis; 5 - umbilical groove: 6 - gallbladder; 7 - right lobe of the liver: 8 - lig. triangulare dextrum; 9 - diaphragm; 10 - lig. coronarium
The falciform ligament is located in the sagittal plane, between the diaphragm and the spherical surface of the liver. Its length is 8-15 cm, width - 3-8 cm. In the anterior part of the liver it continues as a round ligament. In the thickness of the latter there is the umbilical vein, which in the stage of intrauterine development of the fetus connects the placenta with the left branch of the AV. After the birth of a child, this vein is not obliterated, but is in a collapsed state. It is often used for contrast studies of the portal system and the introduction medicinal substances for liver diseases.
The posterior part of the falciform ligament becomes the coronary ligament, which extends from the inferior surface of the diaphragm towards the border lying between the upper and posterior parts of the liver. The coronary ligament extends along the frontal plane. Its upper layer is called the hepatophrenic ligament, and the lower layer is called the hepatorenal ligament. Between the leaves of the coronary ligament there is a part of the liver devoid of peritoneal cover. The length of the coronary ligament ranges from 5 to 20 cm. Its right and left edges turn into triangular ligaments.
Liver topography
The liver is located in the upper abdomen. It is attached to the lower surface of the diaphragm and is covered over a large area with ribs. Only a small part of its anterior surface is attached to the anterior wall of the abdomen. Most of the liver is located in the right hypochondrium, the smaller part is in the epigastric and left hypochondrium. The midline, as a rule, corresponds to the border lying between the two lobes. The position of the liver changes due to changes in body position. It also depends on the degree of intestinal filling, the tone of the abdominal wall and the presence pathological changes.The upper border of the liver on the right is at the level of the 4th intercostal space along the right nipple line. The superior point of the left lobe is located at the level of the 5th intercostal space along the left parasterial line. The anterior inferior edge along the axillary line is at the level of the 10th intercostal space. The anterior edge along the right nipple line corresponds to the costal margin, then it separates from the costal arch and stretches in an oblique direction upward and to the left. In the midline of the abdomen, it is located between the xiphoid process and the navel. The anterior contour of the liver has the shape of a triangle, most of it is covered by the chest wall. The lower edge of the liver only in the epigastric region is outside the boundaries of the costal arch and is covered by the anterior wall of the abdomen. In the presence of pathological processes, especially developmental defects, the right lobe of the liver can reach the pelvic cavity. The position of the liver changes in the presence of fluid in the pleural cavity, tumors, cysts, ulcers, and ascites. As a result of adhesions, the position of the liver also changes, its mobility is limited and surgical intervention becomes difficult.
In the presence of pathological process the anterior edge of the liver emerges from the hypochondrium and is easily palpated. Percussion in the liver area produces a dull sound, on the basis of which it is determined relative boundaries. The upper border of the liver is located at the level of the 5th rib along the midclavicular line, and behind the 10th rib along the scapular line. The lower border along the midclavicular line crosses the costal arch, and along the scapular line reaches the 11th rib.
Blood vessels of the liver
The liver has arterial and venous vascular systems. Blood flows into the liver from the IV and hepatic artery (HA). The main vessels of the arterial system are the common and proper arteries of the liver. The common hepatic artery (CHA) is a branch of the truncus coeliacus with a length of 3-4 cm and a diameter of 0.5-0.8 cm. This artery passes along the upper edge of the pancreas and, reaching the duodenal ligament, divides into the gastroduodenal and proper hepatic arteries . OPA is sometimes divided at the same level into branches of the right and left hepatic and pancreaticoduodenal arteries. The left gastric artery (accompanied by the vein of the same name) passes through the hepatoduodenal ligament next to the PCA.The proper hepatic artery (SPA) runs along the upper part of the hepatoduodenal ligament. It is located in front of the PV, to the left of the common gastric duct (CGD) and somewhat deeper than it. Its length ranges from 0.5 to 3 cm, diameter from 0.3 to 0.6 cm. In the initial section, the right gastric artery is separated from it, which in the anterior part of the porta hepatis is divided into right and left branches (corresponding to the lobes of the liver). The blood flowing through the PA makes up 25% of the blood flow to the liver, and 75% is the blood flowing through the IV.
In some cases, SPA is divided into three branches. The left VA supplies blood to the left, quadrate and caudate lobes of the liver. Its length is 2-3 cm, diameter - 0.2-0.3 cm. Its initial part is located inside the hepatic ducts, in the front part of the IV. The right PA is larger than the left. Its length is 2-4 cm, diameter is 0.2-0.4 cm. It supplies blood to the right lobe of the liver and gallbladder. In the area of the porta hepatis, it crosses the CBD and runs along the anterior and superior part of the PV.
In 25% of cases, SPA begins from the left gastric artery, and in 12% from the superior mesenteric artery. In 20% of cases, it is directly divided into 4 arteries - the gastroduodenal, gastropyloric arteries, right and left VA. In 30% of cases, additional PAs are noted. In some cases, there are three separate VAs: the median, right and left lateral arteries.
The right VA sometimes starts directly from the aorta. The division of the VA into the right and left lobar arteries usually occurs on the left side of the interlobar groove. In some cases, this occurs on the inner side of the left portal sulcus. In this case, the left VA provides blood only to the left “classical” lobe, and the quadrate and caudate lobes receive blood from the right VA.
Venous network of the liver
Represents afferent and efferent blood venous system. The main vein leading to blood is the IV (v. Porta). The outflow of blood from the liver is carried out by the PV. The portal system (Figure 3) collects blood from almost all organs of the abdomen. The PV is formed mainly from the confluence of the superior mesenteric and splenic veins. The PV carries out the outflow of blood from all parts of the gastrointestinal tract, pancreas and spleen. In the area of the porta hepatis, the PV is divided into right and left branches. The PV is located in the thickness of the hepatoduodenal ligament behind the CBD and SPA. Blood through the PV enters the liver and leaves the liver through the PV, which enters the IVC.
Figure 3. Formation of the extrahepatic PV trunk:
1 - right branch of the BB; 2 — left branch of the BB; 3 - accessory vein of the pancreas; 4 - coronary vein of the stomach; 5 - veins of the pancreas; 6 - short veins of the stomach; 7 - splenic veins; 8 - left gastroepiploic vein; 9 — trunk of the splenic vein; 10 - colonic veins; 11 - superior mesenteric vein; 12 - omental vein; 13 - small intestinal veins; 14 - right gastroepiploic vein; 15 - inferior pancreatoduodenal vein; 16 - superior pancreatoduodenal vein; 17 - pyloric vein; 18 - gallbladder vein
The mesenteric and middle colic veins sometimes take part in the formation of the PV trunk. The length of the main trunk of the PV ranges from 2 to 8 cm, and in some cases reaches 14 cm. The PV passes behind the pancreas in 35% of cases, in 42% of cases it is partially localized in the gland tissue, and in 23% of cases in the thickness of its parenchyma. The liver tissue receives a huge amount of blood (84 ml of blood passes through the liver parenchyma in 1 minute). In the PV, as in other vessels, there are sphincters that regulate the movement of blood in the liver. If their function is impaired, the hemodynamics of the liver are also disrupted, as a result of which an obstacle to the outflow of blood may occur and dangerous blood filling of the liver may develop. From the IV, blood passes into the interlobular capillaries, and from there through the PV system into the IVC. The pressure in the PV ranges from 5-10 mmHg. Art. The pressure difference between the initial and final parts is 90-100 mm Hg. Art. Due to this pressure difference, progressive blood flow occurs (V.V. Parii). In a person, on average, 1.5 liters of blood flows through the portal system in 1 minute. The portal system, together with the PV, creates a huge blood depot, which is important for regulating hemodynamics both normally and in the presence of pathological changes. The hepatic vessels can simultaneously accommodate 20% of the total blood volume.
The function of blood deposition contributes to a sufficient supply of more intensively functioning organs and tissues. With major bleeding, against the background of a decrease in blood flow to the liver, there is an active release of blood from the depot into the general bloodstream. In some pathological conditions (shock, etc.), 60-70% of the body’s total blood can accumulate in the portal bed. This phenomenon is conventionally called “bleeding into the abdominal organs.” The PV is connected to the IVC by multiple anastomoses. These include anastomoses between the veins of the stomach, esophagus, PC, anastomoses between the periumbilical vein and the veins of the anterior abdominal wall, etc. These anastomosis play an important role in the disturbance of venous outflow in the portal system. In this case, collateral circulation develops. Porto-caval anastomoses are especially well pronounced in the area of the PC and on the anterior wall of the abdomen. With portal hypertension (PH), anastomoses occur between the gastric and esophageal veins.
If outflow in the portal system is difficult (liver cirrhosis (LC), Budd-Chiari syndrome), blood can pass through these anastomoses from the IV system to the IVC. With the development of PG, varicose dilation of the esophageal-gastric veins occurs, which often causes severe bleeding.
The outflow of venous blood from the liver occurs through the PV.
The PVs consist of three trunks that enter the IVC. The latter is located on the posterior surface of the liver, in the groove of the IVC, between the caudate and right lobes of the liver. It passes between the leaves of the falciform and coronary ligaments. PVs are formed as a result of the fusion of lobular and segmental veins. The number of PVs sometimes reaches 25. However, three veins are predominantly found: right, middle and left. It is believed that the right PV provides the outflow of blood from the right lobe, middle vein- from the quadrate and caudate lobes, and the left vein - from the left lobe of the liver. The liver consists of multiple lobules, which are separated from each other by connective tissue bridges, through which interlobar veins and the smallest branches of the PA, as well as lymphatic vessels and nerves pass. Approaching the liver lobules, the branches of the PV form interlobar veins, which then, turning into septal veins, are connected through anastomoses to the veins of the IVC system. From the septal veins, sinusoids are formed, which enter the central vein. PAs are also divided into capillaries, which enter the lobule and in its peripheral part connect with small veins. The sinusoids are covered with endothelium and macrophages (Kupffer cells).
The outflow of lymph from the liver into the thoracic lymphatic duct occurs in three directions. In some cases, lymph flowing from the hepatic parenchyma enters the mediastinal lymph nodes.
Innervation of the liver carried out from the right visceral nerve and parasympathetic nerve fibers emanating from the hepatic branches of the vagus nerve. There are anterior and posterior hepatic plexuses, which are formed from the solar plexus. The anterior nerve plexus is located between the two layers of the lesser omentum, along the VA. The posterior hepatic plexus is formed from preganglionic nerve fibers of the solar plexus and the borderline trunk.
Liver functions
The liver plays a very important role in the processes of digestion and interstitial metabolism. The role of the liver is especially important in the process of carbohydrate metabolism. Sugar entering the liver through the IV is converted into glycogen (glycogen synthesizing function). Glycogen is stored in the liver and used according to the body's needs. The liver actively regulates peripheral blood sugar levels.The liver also plays a great role in neutralizing tissue breakdown products, various types of toxins and products of interstitial metabolism (antitoxic function). The antitoxic function is complemented by the excretory function of the kidneys. The liver neutralizes toxic substances, and the kidneys excrete them in a less toxic state. The liver also performs a protective function and plays the role of a kind of barrier.
The role of the liver is also great in protein metabolism. The liver synthesizes amino acids, urea, hippuric acid and plasma proteins, as well as prothrombin, fibrinogen, etc.
The liver is involved in fat and lipid metabolism, it produces the synthesis of cholesterol, lecithins, fatty acids, the absorption of exogenous fats, the formation of phospholipids, etc. The liver is involved in the production of bile pigments, in the circulation of urobilin (liver—biliary tract—portal system—liver bile) (bile-forming function). In many liver diseases, pigment function is more often affected.
Hepar, the largest of the digestive glands, occupies the upper abdominal cavity, located under the diaphragm, mainly on the right side.
By shape liver somewhat resembles the cap of a large mushroom, has an upper convex and lower slightly concave surface. However, the convexity is devoid of symmetry, since the most protruding and voluminous part is not the central, but the right rear, which tapers anteriorly and to the left in a wedge-shaped manner. Human liver dimensions: from right to left on average 26-30 cm, from front to back - right lobe 20-22 cm, left lobe 15-16 cm, greatest thickness (right lobe) - 6-9 cm. The weight of the liver is on average 1500 g. Its color is red -brown, soft consistency.
Structure human liver: there is a convex upper diaphragmatic surface, facies diaphragmatica, a lower, sometimes concave, visceral surface, facies visceralis, a sharp lower edge, margo inferior, separating the upper and lower surfaces in front, and a slightly convex rear part, pars posterior. diaphragmatic surface.
On the lower edge of the liver there is a notch of the round ligament, incisura ligaments teretis: to the right there is a small notch corresponding to the adjacent bottom of the gallbladder.
The diaphragmatic surface, facies diaphragmatica, is convex and corresponds in shape to the dome of the diaphragm. From the highest point there is a gentle slope to the lower sharp edge and to the left, to the left edge of the liver; a steep slope follows to the posterior and right parts of the diaphragmatic surface. Upwards, to the diaphragm, there is a sagittally located peritoneal falciform ligament of the liver, lig. falciforme hepatis, which follows from the lower edge of the liver back for about 2/3 of the width of the liver: behind the leaves of the ligament diverge to the right and left, passing into the coronary ligament of the liver, lig. coronarium hepatis. The falciform ligament divides the liver, according to its upper surface, into two parts - the right lobe of the liver, lobus hepatis dexter, which is large and has the greatest thickness, and the left lobe of the liver, lobus hepatis sinister, which is smaller. On the upper part of the liver one can see a small cardiac depression, impressio cardiaca, formed as a result of the pressure of the heart and corresponding to the tendon center of the diaphragm.

On the diaphragm liver surface distinguish the upper part, pars superior, facing the tendon center of the diaphragm; the anterior part, pars anterior, facing anteriorly, to the costal part of the diaphragm, and to the anterior wall of the abdomen in the epigastric region (left lobe); the right part, pars dextra, directed to the right, towards the lateral abdominal wall (corresponding to the mid-axillary line), and the back part, pars posterior, facing towards the back.

The visceral surface, facies visceralis, is flat, slightly concave, corresponding to the configuration of the underlying organs. There are three grooves on it, dividing this surface into four lobes. Two grooves have a sagittal direction and stretch almost parallel to one another from the anterior to the posterior edge of the liver; approximately in the middle of this distance they are connected, as if in the form of a crossbar, by a third, transverse, furrow.
The left sulcus consists of two sections: the anterior, extending to the level of the transverse sulcus, and the posterior, located posterior to the transverse. The deeper anterior section is the fissure of the round ligament, fissura lig. teretis (in the embryonic period - the groove of the umbilical vein), begins on the lower edge of the liver from the notch of the round ligament, incisura lig. teretis. it contains the round ligament of the liver, lig. teres hepatis, running in front and below the navel and enclosing the obliterated umbilical vein. The posterior part of the left groove is the fissure of the venous ligament, fissura lig. venosi (in the embryonic period - fossa ductus venosi, fossa ductus venosi), contains the venous ligament, lig. venosum (obliterated ductus venosus), and stretches from the transverse groove back to the left hepatic vein. The left groove, in its position on the visceral surface, corresponds to the line of attachment of the falciform ligament on the diaphragmatic surface of the liver and, thus, serves here as the boundary of the left and right lobes of the liver. At the same time, the round ligament of the liver is located in the lower edge of the falciform ligament, on its free anterior section.
The right groove is a longitudinally located fossa and is called the gallbladder fossa, fossa vesicae felleae, which corresponds to a notch on the lower edge of the liver. It is less deep than the groove of the round ligament, but wider and represents the imprint of the gallbladder located in it, vesica fellea. The fossa extends posteriorly to the transverse groove; its continuation posterior to the transverse groove is the groove of the inferior vena cava, sulcus venae cavae inferioris.
The transverse groove is the gate of the liver, porta hepatis. It contains the own hepatic artery, a. hepatis propria, common hepatic duct, ductus hepaticus communis, and portal vein, v. portae.
Both artery and vein are divided into main branches, right and left, already at the hilum liver.

These three grooves divide the visceral surface of the liver into four lobes of the liver, lobi hepatis. The left groove delimits the lower surface of the left lobe of the liver to the right; the right groove demarcates on the left the lower surface of the right lobe of the liver.
The middle area between the right and left grooves on the visceral surface of the liver is divided by a transverse groove into anterior and posterior. The anterior portion is the quadrate lobe, lobus quadratus, and the posterior portion is the caudate lobe, lobus caudatus.
On the visceral surface of the right lobe of the liver, closer to the anterior edge, there is a colonic depression, impressio colica; behind, to the very rear edge, there are: to the right - a large depression from the right kidney adjacent here, the renal depression, impressio renalis, to the left - the duodenal (duodenal) depression, impressionio duodenalis, adjacent to the right groove; even more posteriorly, to the left of the renal depression, - depression of the right adrenal gland, adrenal depression, impressio suprarenalis.
The square lobe of the liver, lobus quadratus hepatis, is bounded on the right by the fossa, on the left by the fissure of the round ligament, in front by the lower edge, and behind by the porta hepatis. In the middle of the width of the square lobe there is a depression in the form of a wide transverse groove - an imprint of the upper part, a duodenal indentation that continues here from the right lobe of the liver.
The caudate lobe of the liver, lobus caudatus hepatis, is located posterior to the portal of the liver, limited in front by the transverse groove of the portal of the liver, on the right - by the groove of the vena cava, sulcus venae cavae, on the left - by the fissure of the venous ligament, fissura lig. venosi, and behind - the posterior part of the diaphragmatic surface of the liver. On the anterior section of the caudate lobe on the left there is a small protrusion - the papillary process, processus papillaris, adjacent to the back of the left part of the porta hepatis; on the right, the caudate lobe forms the caudate process, processus caudatus, which goes to the right, forms a bridge between the posterior end of the gallbladder fossa and the anterior end of the groove of the inferior vena cava and passes into the right lobe of the liver.
The left lobe of the liver, lobus hepatis sinister, on the visceral surface, closer to the anterior edge, has a convexity - the omental tubercle, tuber omentale, which faces the lesser omentum, omentum minus. On the posterior edge of the left lobe, immediately next to the fissure of the venous ligament, there is a depression from the adjacent abdominal part of the esophagus - the esophageal depression, impressio esophageale.
To the left of these formations, closer to the back, on the lower surface of the left lobe there is a gastric impression, impressio gastrica.
The posterior part of the diaphragmatic surface, pars posterior faciei diaphragmaticae, is a rather wide, slightly rounded section of the surface of the liver. It forms a concavity corresponding to the place of contact with the spine. Its central section is wide, and narrows to the right and left. Corresponding to the right lobe there is a groove in which the inferior vena cava is located - the groove of the vena cava, sulcus venae cavae. Closer to the upper end of this groove in the substance of the liver, three hepatic veins, venae hepaticae, are visible, flowing into the inferior vena cava. The edges of the groove of the vena cava are connected to each other by the connective tissue ligament of the inferior vena cava.
The liver is almost completely surrounded by the peritoneum. The serous membrane, tunica serosa, covers its diaphragmatic, visceral surfaces and lower edge. However, in places where the ligaments approach the liver and the gallbladder is adjacent, there remain areas of varying widths that are not covered by the peritoneum. The largest area not covered by peritoneum is on the posterior part of the diaphragmatic surface, where the liver is directly adjacent to the posterior wall of the abdomen; it has the shape of a rhombus - extraperitoneal field, area nuda. Corresponding to its greatest width, the inferior vena cava is located. The second such area is located at the location of the gallbladder. The peritoneal ligaments extend from the diaphragmatic and visceral surfaces of the liver.
The structure of the liver.
The serous membrane, tunica serosa, covering the liver, is underlain by the subserosal base, tela subserosa, and then by the fibrous membrane, tunica fibrosa. Through the portal of the liver and the posterior end of the gap of the round ligament, together with the vessels, connective tissue penetrates into the parenchyma in the form of the so-called perivascular fibrous capsule, capsula fibrosa perivascularis, in the processes of which are located the branches of the portal vein and the proper hepatic artery; along the course of the vessels it reaches the fibrous membrane from the inside. This is how a connective tissue frame is formed, in the cells of which the liver lobules are located.

Liver lobule.
Liver lobule, lobulus hepaticus, 1-2 mm in size. consists of liver cells - hepatocytes, hepatocyti, forming liver plates, laminae hepaticae. In the center of the lobule is the central vein, v. centralis, and around the lobule there are interlobular arteries and veins, aa. interlobular et vv, interlobulares, from which interlobular capillaries originate, vasa capillaria interlobularia. Interlobular capillaries enter the lobule and pass into sinusoidal vessels, vasa sinusoidea, located between the hepatic plates. In these vessels arterial and venous (from v, portae) blood mixes. The sinusoid vessels empty into the central vein. Each central vein joins the sublobular, or collecting, veins, vv. sublobulares, and the latter - into the right, middle and left hepatic veins. vv. hepaticae dextrae, mediae et sinistrae.
Between the hepatocytes lie bile canaliculi, canaliculi biliferi, which flow into the ductuli biliferi, and the latter, outside the lobules, connect into the ductus interlobulares biliferi. Segmental ducts are formed from the interlobular bile ducts.
Based on the study of intrahepatic vessels and bile ducts, a modern understanding of the lobes, sectors and segments of the liver has emerged. The branches of the portal vein of the first order bring blood to the right and left lobes of the liver, the border between which does not correspond to the external border, but passes through the fossa of the gallbladder and the groove of the inferior vena cava.

Second-order branches provide blood flow to the sectors: in the right lobe - to the right pyramidal sector, sector paramedianum dexter, and the right lateral sector, sector lateralis dexter; in the left lobe - into the left paramedian sector, sector paramedianum sinister, the left lateral sector, sector lateralis sinister, and the left dorsal sector, sector dorsalis sinister. The last two sectors correspond to liver segments I and II. The other sectors are each divided into two segments, so that there are 4 segments in the right and left lobes.
The lobes and segments of the liver have their own bile ducts, branches of the portal vein and their own hepatic artery. The right lobe of the liver is drained by the right hepatic duct, ductus hepaticus dexter, which has anterior and posterior branches, r. anterior et r. posterior, the left lobe of the liver - the left hepatic duct, ductus hepaticus sinister, consisting of medial and lateral branches, r. medialis et lateralis, and the caudate lobe - by the right and left ducts of the caudate lobe, ductus lobi caudati dexter et ductus lobi caudati sinister.
The anterior branch of the right hepatic duct is formed from the ducts of segments V and VIII; the posterior branch of the right hepatic duct - from the ducts of segments VI and VII; the lateral branch of the left hepatic duct is from the ducts of segments II and III. The ducts of the quadrate lobe of the liver flow into the medial branch of the left hepatic duct - the duct of the IV segment, and the right and left ducts of the caudate lobe, the ducts of the I segment can flow together or separately into the right, left and common hepatic ducts, as well as into the posterior branch of the right and into the lateral branch left hepatic duct. There may be other options for connecting segmental ducts I-VIII. The ducts of segments III and IV are often connected.
The right and left hepatic ducts at the anterior edge of the porta hepatis or already in the hepatoduodenal ligament form the common hepatic duct, ductus hepaticus communis.
The right and left hepatic ducts and their segmental branches are not permanent structures; if they are absent, then the ducts forming them flow into the common hepatic duct. The length of the common hepatic duct is 4-5 cm, its diameter is 4-5 cm. Its mucous membrane is smooth and does not form folds.
Topography of the liver.
Topography of the liver. The liver is located in the right hypochondrium, in the epigastric region and partially in the left hypochondrium. Skeletotopically, the liver is determined by its projection onto the chest walls. On the right and in front along the midclavicular line, the highest point of the liver (right lobe) is determined at the level of the fourth intercostal space; to the left of the sternum, the highest point (left lobe) is at the level of the fifth intercostal space. The lower edge of the liver on the right along the mid-axillary line is determined at the level of the tenth intercostal space; further forward the lower border of the liver follows the right half of the costal arch. At the level of the right midclavicular line, it emerges from under the arch, goes from right to left and upward, crossing the epigastric region. White line abdomen, the lower edge of the liver crosses midway between the xiphoid process and the umbilical ring. Further, at the level of VIII of the left costal cartilage, the lower border of the left lobe crosses the costal arch to meet the upper border to the left of the sternum.
Colon. It is also adjacent to the internal surface of the right lobe of the liver.
You might be interested in this read:
Reading time: 9 min.
It is important to understand that the liver nerve endings no, that's why she can't be sick. However, pain in the liver area may indicate liver dysfunction. After all, even if the liver itself does not hurt, the organs around it, for example, when it is enlarged or dysfunctional (accumulation of bile), can hurt.
Let's take a closer look at the structure of the liver.
Hepar ( translated from Greek means “Liver”), is a voluminous glandular organ, the mass of which reaches approximately 1,500 g.
First of all, the liver is a gland that produces bile, which then flows through the excretory duct into the duodenum.
In our body, the liver performs many functions. The main ones are: metabolic, responsible for metabolism, barrier, excretory.
Barrier function: is responsible for neutralizing in the liver toxic products of protein metabolism that enter the liver with the blood. In addition, the endothelium of the hepatic capillaries and stellate reticuloendotheliocytes have phagocytic properties, which contributes to the neutralization of substances absorbed in the intestine.
The liver is involved in all types of metabolism; in particular, carbohydrates absorbed by the intestinal mucosa are converted in the liver into glycogen (“glycogen depot”).
Among other things, the liver is also attributed hormonal function.
Works in small children and embryos hematopoietic function ( red blood cells are produced).
Simply put, our liver has the abilities of blood circulation, digestion, and metabolism. different types, including hormonal.
To maintain liver function, you must adhere to proper diet(for example, table No. 5). If organ dysfunction is observed, the use of hepatoprotectors is recommended (as prescribed by a doctor).
The liver itself is located just below the diaphragm, on the right, in the upper part of the abdominal cavity.
Only a small part of the liver extends to the left in an adult. In newborn babies, the liver occupies most of the abdominal cavity or 1/20 of the total body weight (in an adult the ratio is about 1/50).
Let us consider in more detail the location of the liver relative to other organs:
In the liver, it is customary to distinguish 2 edges and 2 surfaces.
Upper surface of the liver is convex relative to the concave shape of the diaphragm to which it is adjacent.
Lower surface of the liver, facing backward and downward and has impressions from the adjacent abdominal viscera.
The upper surface is separated from the lower by a sharp lower edge, margo inferior.
The other edge of the liver, the superoposterior, on the contrary, is so blunt that it is considered as the surface of the liver.


In the structure of the liver, it is customary to distinguish two lobes: the right (larger), lobus hepatis dexter, and the smaller left, lobus hepatis sinister.
On the diaphragmatic surface, these two lobes are separated by the falciform ligament - lig. falciforme hepatis.
The free edge of this ligament contains a dense fibrous cord - the circular ligament of the liver, lig. teres hepatis, which stretches from the navel, umbilicus, and is an overgrown umbilical vein, v. umbilicalis.
The round ligament bends over the lower edge of the liver, forming a notch, incisura ligamenti teretis, and lies on the visceral surface of the liver in the left longitudinal groove, which on this surface is the boundary between the right and left lobes of the liver.
The round ligament occupies the anterior section of this groove - fissiira ligamenti teretis; the posterior section of the groove contains a continuation of the round ligament in the form of a thin fibrous cord- overgrown venous duct, ductus venosus, functioning in the embryonic period of life; this section of the groove is called fissura ligamenti venosi.
The right lobe of the liver on the visceral surface is divided into secondary lobes by two grooves, or depressions. One of them runs parallel to the left longitudinal groove and in the anterior section, where the gallbladder is located, vesica fellea, is called fossa vesicae felleae; the posterior section of the groove, deeper, contains the inferior vena cava, v. cava inferior, and is called sulcus venae cavae.
Fossa vesicae felleae and sulcus venae cavae are separated from each other by a relatively narrow isthmus of liver tissue called the caudate process, processus caudatus.

The deep transverse groove connecting the posterior ends of fissurae ligamenti teretis and fossae vesicae felleae is called porta hepatis, porta hepatis. Through them enter a. hepatica and v. portae with the accompanying nerves and the lymphatic vessels and ductus hepaticus communis, which carries bile from the liver, emerge.
The part of the right lobe of the liver, limited posteriorly by the porta hepatis, laterally by the fossa of the gallbladder on the right and the fissure of the round ligament on the left, is called the quadrate lobe, lobus quadratus. The area posterior to the gate of the liver between the fissura ligamenti venosi on the left and the sulcus venae cavae on the right constitutes the caudate lobe, lobus caudatus.
Organs in contact with the surfaces of the liver form depressions on it, impressiones, which are called the organ in contact.

The liver is covered for most of its length by peritoneum, with the exception of part of its posterior surface, where the liver is directly adjacent to the diaphragm.
The structure of the liver. Beneath the serous membrane of the liver is a thin fibrous membrane, tunica fibrosa. In the area of the portal of the liver, together with the vessels, it enters the substance of the liver and continues into the thin layers of connective tissue surrounding the lobules of the liver, lobuli hepatis.

In humans, the lobules are weakly separated from each other; in some animals, such as pigs, the connective tissue layers between the lobules are more pronounced. Liver cells in the lobule are grouped in the form of plates, which are located radially from the axial part of the lobule to the periphery.
Inside the lobules in the wall of the hepatic capillaries, in addition to endothelial cells, there are stellate cells with phagocytic properties. The lobules are surrounded by interlobular veins, venae interlobulares, which are branches of the portal vein, and interlobular arterial branches, arteriae interlobulares (from a. hepatica propria).
Between the liver cells, which make up the liver lobules, located between the contacting surfaces of two liver cells, there are bile ducts, ductuli biliferi. Coming out of the lobules, they flow into the interlobular ducts, ductuli interlobulares. An excretory duct emerges from each lobe of the liver.
From the confluence of the right and left ducts, the ductus hepaticus communis is formed, which carries bile from the liver, bilis, and emerges from the portal of the liver.
Common hepatic duct most often consists of two ducts, but sometimes of three, four and even five.
Topography of the liver. The liver is projected onto the anterior abdominal wall in the epigastric region. The borders of the liver, upper and lower, projected onto the anterolateral surface of the body, converge with one another at two points: on the right and on the left.
Upper border of the liver begins in the tenth intercostal space on the right, along the midaxillary line. From here it rises steeply upward and medially, corresponding to the projection of the diaphragm, to which the liver is adjacent, and along the right nipple line reaches the fourth intercostal space; from here the border gently descends to the left, crossing the sternum slightly above the base of the xiphoid process, and in the fifth intercostal space it reaches the middle of the distance between the left sternum and left nipple lines.
Bottom line, starting in the same place in the tenth intercostal space as upper bound, goes from here obliquely and medially, crosses the IX and X costal cartilages on the right, goes along the epigastric region obliquely to the left and up, crosses the costal arch at the level of the VII left costal cartilage and in the fifth intercostal space connects with the upper border.
Ligaments of the liver. The liver ligaments are formed by the peritoneum, which passes from the lower surface of the diaphragm to the liver, to its diaphragmatic surface, where it forms the coronary ligament of the liver, lig. coronarium hepatis. The edges of this ligament have the form of triangular plates, designated as triangular ligaments, ligg. triangulare dextrum et sinistrum. Ligaments extend from the visceral surface of the liver to the nearest organs: to the right kidney - lig. hepatorenale, to the lesser curvature of the stomach - lig. hepatogastricum and to duodenum- lig. hepatoduodenal.
Liver nutrition occurs due to a. hepatica propria, but in a quarter of cases from the left gastric artery. The peculiarities of the liver vessels are that, in addition to arterial blood, it also receives venous blood. Through the gate, a. enters the substance of the liver. hepatica propria and v. portae. Entering the gate of the liver, v. portae, carrying blood from the unpaired organs of the abdominal cavity, branches into the thinnest branches located between the lobules - vv. interlobulares. The latter are accompanied by aa. interlobulares (branches a. hepatica propia) and ductuli interlobulares.
In the substance of the liver lobules themselves, capillary networks are formed from arteries and veins, from which all the blood collects in the central veins - vv. centrales. Vv. centrales, leaving the liver lobules, flow into the collecting veins, which, gradually connecting with each other, form vv. hepaticae. The hepatic veins have sphincters where they join the central veins. Vv. hepaticae in the amount of 3-4 large and several small ones emerge from the liver on its posterior surface and flow into the v. cava inferior.
Thus, in the liver there are two systems of veins:
- portal, formed by branches v. portae, through which blood flows into the liver through its gate,
- caval, representing the totality of vv. hepaticae, carrying blood from the liver to v. cava inferior.
In the uterine period, another third functions, umbilical vein system; the latter are branches of v. umbilicalis, which obliterates after birth.
As for the lymphatic vessels, there are no true lymphatic capillaries inside the liver lobules: they exist only in the interglobular connective tissue and flow into the plexus of lymphatic vessels accompanying the branches of the portal vein, hepatic artery and bile ducts, on the one hand, and the roots of the hepatic veins, on the other . The efferent lymphatic vessels of the liver go to the nodi hepatici, coeliaci, gastrici dextri, pylorici and to the peri-aortic nodes in the abdominal cavity, as well as to the phrenic and posterior mediastinal nodes (in the chest cavity). About half of the body's lymph is drained from the liver.
Innervation of the liver carried out from the celiac plexus through truncus sympathicus and n. vagus
Segmental structure of the liver. In connection with the development of surgery and the development of hepatology, the doctrine of the segmental structure of the liver has now been created, which has changed the previous idea of \u200b\u200bdividing the liver only into lobes and segments. As noted, the liver has five tubular systems:
- bile ducts,
- arteries,
- branches of the portal vein (portal system),
- hepatic veins (caval system)
- lymphatic vessels.
The portal and caval vein systems do not coincide with each other, and the remaining tubular systems accompany the branches of the portal vein, run parallel to each other and form vascular-secretory bundles, to which nerves are attached. Some of the lymphatic vessels exit along with the hepatic veins.

Liver segment- this is a pyramidal section of its parenchyma adjacent to the so-called hepatic triad: a branch of the portal vein of the 2nd order, an accompanying branch of the proper hepatic artery and the corresponding branch of the hepatic duct.
The following segments are distinguished in the liver, starting from the sulcus venae cavae to the left, counterclockwise:
- I - caudate segment of the left lobe, corresponding to the conominal lobe of the liver;
- II - posterior segment of the left lobe, localized in the posterior part of the lobe of the same name;
- III - anterior segment of the left lobe, located in its department of the same name;
- IV - square segment of the left lobe, corresponds to the conominal lobe of the liver;
- V - middle upper anterior segment of the right lobe;
- VI - lateral inferoanterior segment of the right lobe;
- VII - lateral infero-posterior segment of the right lobe;
- VIII - middle superoposterior segment of the right lobe. (Segment names indicate areas of the right lobe.)
Let's take a closer look at the segments (or sectors) of the liver:

In total, it is customary to divide the liver into 5 sectors.
- The left lateral sector corresponds to segment II (monosegmental sector).
- The left paramedian sector is formed by segments III and IV.
- The right paramedian sector consists of segments V and VIII.
- The right lateral sector includes segments VI and VII.
- The left dorsal sector corresponds to segment I (monosegmental sector).
By the time of birth, the liver segments are clearly defined, because are formed are formed in the uterine period.
The doctrine of the segmental structure of the liver is more detailed and profound compared to the idea of dividing the liver into lobules and lobes.


