Antipyretics for children are prescribed by a pediatrician. But there are emergency situations with fever when the child needs to be given medicine immediately. Then the parents take responsibility and use antipyretic drugs. What is allowed to be given to infants? How can you lower the temperature in older children? What medications are the safest?
A bruise is a type of closed bruise in which the superficial soft tissues are damaged ( , subcutaneous fat, small vessels, muscles, etc.) bodies without violating their anatomical integrity ( that is, without the formation of wounds). Shoulder bruises are quite often combined with other types of injuries - bones, joints, muscle inflammation ( ), joints ( ), violation of the integrity of ligaments, tendons, nerve damage, etc.
Shoulder bruises most often occur when falling on the shoulder area, colliding with hard objects, as well as after direct blows to the shoulder, heavy bodies falling on the shoulder, etc. The appearance of a shoulder bruise is always accompanied by the appearance of intense swelling at the site of injury, impaired mobility in one or more several joints. On the skin at the site of injury, redness first appears, and then bruising ( ), petechiae ( intradermal pinpoint hemorrhages). With more severe bruises, hematomas may occur on the shoulder ( cavities filled with blood), impaired skin sensitivity.
Anatomy of the shoulder area
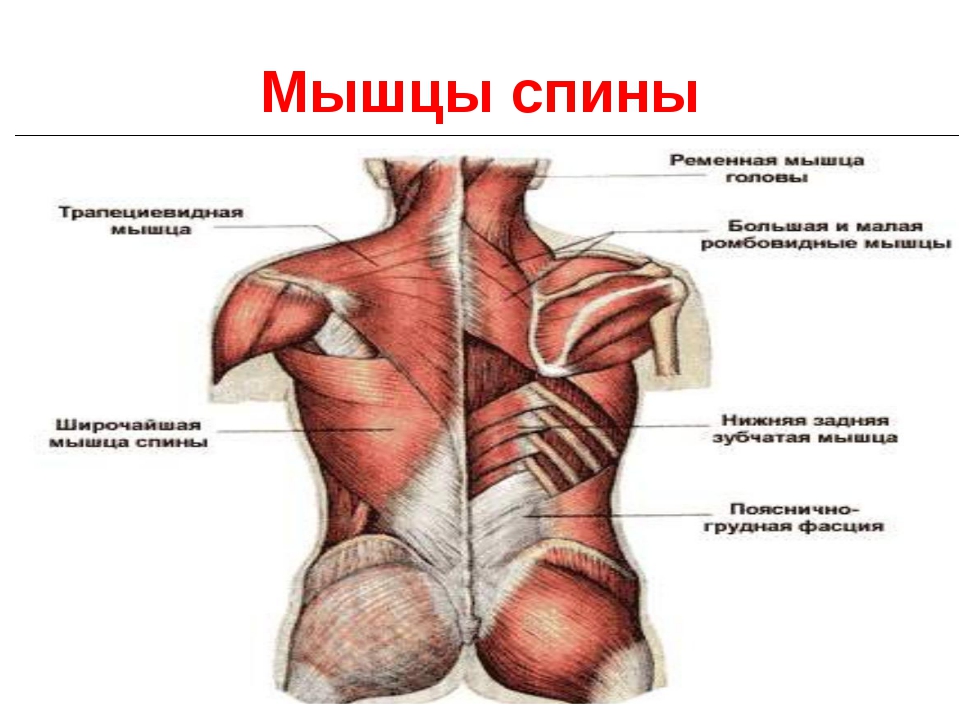
 The shoulder is the initial part of the human upper limb. It is located between the shoulder and elbow joints of the arm. Like all other open areas of the body, the shoulder is covered on the outside with skin and subcutaneous fat. The muscles are located deeper than them. All shoulder muscles are divided into anterior ( coracobrachialis, brachialis, biceps, muscles) and back ( articular muscle of the elbow, triceps, anconeus muscles) groups. These muscles allow you to manipulate the forearm and make various movements in it. In addition to these muscles at the top of the shoulder, the muscles of the shoulder girdle are connected to it ( supraspinatus, infraspinatus, teres minor, deltoid, etc.), which, in turn, help the arm perform certain actions in the shoulder joint.
The shoulder is the initial part of the human upper limb. It is located between the shoulder and elbow joints of the arm. Like all other open areas of the body, the shoulder is covered on the outside with skin and subcutaneous fat. The muscles are located deeper than them. All shoulder muscles are divided into anterior ( coracobrachialis, brachialis, biceps, muscles) and back ( articular muscle of the elbow, triceps, anconeus muscles) groups. These muscles allow you to manipulate the forearm and make various movements in it. In addition to these muscles at the top of the shoulder, the muscles of the shoulder girdle are connected to it ( supraspinatus, infraspinatus, teres minor, deltoid, etc.), which, in turn, help the arm perform certain actions in the shoulder joint. Deeper than the muscles in the shoulder region there is one single bone ( brachial bone), which connects at the top ( through the head humerus ) with the scapula, forms the shoulder joint. From below it contacts the bones of the forearm ( radial and ulnar), forming elbow joint.
The shoulder blade is classified as a bone of the shoulder girdle. It, together with the clavicle, provides the connection between the bones of the upper limb and the bones of the torso.
Each joint ( elbow or shoulder) is covered on top with a connective tissue membrane called the joint capsule. This capsule limits the joint from other tissues and also stabilizes the articular surfaces of the bones that form it. The articular surfaces of each bone are covered with hyaline cartilage, which ensures optimal sliding between them and cushions movement in the joint.
In addition to the articular capsule, each joint is strengthened by the ligamentous apparatus. Joint ligaments are made of strong connective tissue. They can be located both outside and inside the articular cavity of the joints. To the bundles shoulder joint include three articular-brachial ligaments and the coracobrachial ligament. The elbow joint is firmly fixed by the ulnar and radial collateral ligaments, as well as the quadrate and annular ligaments of the radius.
Near ( above) the acromioclavicular joint is located with the shoulder joint. This joint is the connection between the acromion ( bony process) scapula and the humeral end of the clavicle. This joint is strengthened by the coracoclavicular and acromioclavicular ligaments. The acromioclavicular joint is a low-moving joint.
Oxygenated arterial blood enters the upper extremities through the axillary arteries. These arteries serve as a direct continuation of the subclavian arteries arising from the aorta ( the right subclavian artery arises from the aortic arch through the brachiocephalic trunk). The aorta is the main arterial vessel into which blood enters after passing through.
Both axillary arteries ( right and left) turn into brachial arteries, supplying blood to most of the shoulder. Thus, the main main vessels that bring blood to the tissues of the shoulder of each arm are the axillary and brachial arteries. They both pass along the medial ( inner side) hand surface. The axillary artery is localized in the axillary region, and the brachial artery is localized near the medial ( internal side) edges of the humerus.
Venous blood from the shoulder area is removed through the superficial ( lateral and medial subcutaneous) and deep veins. Superficial veins are located directly under the skin and subcutaneous fat. The deep veins pass under the muscles and are adjacent to the brachial artery along the entire length of the shoulder. The superficial and deep veins in the upper region of the shoulder join together, creating the so-called axillary vein, which then flows into the subclavian vein.
All nerves that innervate the shoulder area ( as well as the shoulder girdle), arise from the brachial nerve plexus. This plexus is formed by connecting several ( fifth, sixth, seventh, eighth, etc.) cervical spinal nerves. The branches of the brachial plexus are anatomically divided into two parts. The part of it that is located above the collarbone is called supraclavicular. At this level, nerves emerge from the brachial plexus ( suprascapular, subclavian, etc.), innervating the muscles of the shoulder girdle, neck, chest and back.
Having given off its supraclavicular branches above the clavicle, the brachial plexus then follows under it and passes from its inner side, heading towards the shoulder. Below the collarbone, subclavian branches extend from the brachial plexus, innervating various tissues ( muscles, skin, joint formations, etc.) of the upper limb, as well as certain muscles of the chest, shoulder girdle, back and chest. The shoulder is innervated by the lateral ( lateral root of the median nerve, musculocutaneous nerve), rear ( radial and axillary nerves), medial ( medial cutaneous nerve of the shoulder, ulnar nerve, medial root of the median nerve) bundles of nerves branching from the brachial plexus.
What structures can be damaged in a shoulder injury?
 With simple bruises, as a rule, more superficial layers are damaged - skin, subcutaneous fat, and less often - muscles, their tendons or ligaments. With serious bruises, damage to deeper anatomical formations quite often occurs - joints, bones, nerves, blood vessels.
With simple bruises, as a rule, more superficial layers are damaged - skin, subcutaneous fat, and less often - muscles, their tendons or ligaments. With serious bruises, damage to deeper anatomical formations quite often occurs - joints, bones, nerves, blood vessels. When a shoulder is bruised, the following anatomical structures can be damaged:
- Skin and subcutaneous tissue. Skin and subcutaneous tissue are the main structures that are damaged by bruises.
- Muscles. Muscles are often damaged by moderate to severe bruises. They can also be affected by various complications of shoulder contusions ( fractures, dislocations, damage to nerves, blood vessels, etc.).
- Muscle tendons. Muscle tendons are often damaged by bruises, complicated by fractures of the humerus or shoulder dislocations.
- Bones. Bones are usually damaged by bruises associated with fractures or joint dislocations. With open fractures, suppuration may occur in the bones ( ) due to infection of the wound site with pathogenic.
- Joint structures. When a shoulder is bruised, shoulder dislocation, intra-articular bone fracture, or inflammation of the joint can sometimes occur. It is in these cases that damage to the articular structures occurs ( joint capsule, cartilage, bursae, ligaments).
- Nerves and blood vessels. Nerves and blood vessels are often damaged during bruises due to direct mechanical trauma ( impact, rupture, etc.) or because they are injured indirectly ( when mixing bone fragments during bone fractures, joint dislocation, etc.).
The main causes of shoulder pain due to injury
 A bruise is one of the types of traumatic injuries in which there is damage to soft tissues that develops under the influence of an external force. Shoulder bruises are usually observed after direct violence, that is, after blows to this area, falls on it, collision of the shoulder with solids, something heavy falls on this area. The severity of a bruise always depends on the mass, type, speed of the traumatic agent, as well as the area of damage to the tissues of the shoulder.
A bruise is one of the types of traumatic injuries in which there is damage to soft tissues that develops under the influence of an external force. Shoulder bruises are usually observed after direct violence, that is, after blows to this area, falls on it, collision of the shoulder with solids, something heavy falls on this area. The severity of a bruise always depends on the mass, type, speed of the traumatic agent, as well as the area of damage to the tissues of the shoulder. With a mild and superficial bruise of the shoulder, damage to the skin, small vessels and subcutaneous fat is noted, nerve endings and, to a lesser extent, muscles and ligaments. Quite often, small vessels at the site of injury can be destroyed. This leads to minor bleeding in the skin, which looks like petechiae ( pinpoint hemorrhages up to 1 – 2 mm in diameter). Petechiae in their size and preferential localization in tissues differ from another type of hemorrhage - ecchymosis.
Ecchymoses ( bruises or bruises) are significant subcutaneous hemorrhages. They develop in the area of subcutaneous fat. With them, it is saturated with blood, while the accumulation of blood as such does not occur in it. Often, with ecchymosis, the skin and/or muscles can become saturated along with subcutaneous fat. In some cases, with severe bruises of the shoulder, blood can accumulate in the subcutaneous fat, forming a hematoma ( cavity inside tissue filled with blood).
Bruises after a shoulder injury are very well recognized on the 2nd - 3rd day in the form of blue ( blue-purple) spots ( in some cases they may appear within a few minutes or hours from the moment of injury). As blood elements disintegrate in the tissues, these spots acquire a green and then a yellow tint. A color change from blue to green or yellow begins to occur from 4 to 10 days after the injury. Until then, the site of injury usually remains bluish. With a mild and superficial injury to the shoulder, the bruises resolve after 12 to 16 days.
Characteristic signs of a shoulder injury are also considered to be swelling and pain at the site of injury. The pain syndrome from a shoulder injury is usually caused either by direct damage to the nerve endings located in the tissues of the shoulder, or by their compression due to increasing swelling of these tissues ( nerves can be compressed and cause hematoma). Edema ( swelling) shoulder tissues are caused by their inflammation. Inflammation is a pathological response of the body to damage or destruction of its tissues. It is accompanied by a local dilation of small vessels, an increase in their permeability, and an increase in blood flow to the affected tissues. All this is the reason why they develop.
With severe bruises of the shoulder area, deeper structures may also be damaged ( bones, joints, ligaments, muscles). This is why shoulder contusions are often associated with other types of shoulder injuries. The presence of an additional type of injury contributes to the occurrence of even more severe pain and even more pronounced swelling of the shoulder.
Shoulder bruises can be combined with the following types of injuries:
- fracture of the humerus, scapula, clavicle;
- dislocation of the shoulder, collarbone;
- muscle inflammation;
- inflammation of the shoulder or elbow joint;
- tendon damage;
- damage peripheral nerves;
- open shoulder injuries.
Fracture of humerus, scapula, clavicle
Fracture of the humerus, scapula, and collarbone is a common occurrence with bruises in the shoulder area. When fractures occur, partial or complete destruction of the anatomical structure of the bones occurs. Such fractures usually occur as a result of a fall on the elbow joint, shoulder, or a direct blow to the shoulder area. A fracture of these bones is characterized by the appearance severe pain and swelling in the area of damage, as well as the occurrence of pathological mobility ( the presence of mobility in a place where it is not normally detected), crepitation ( crunch of bone fragments), joint dysfunction ( elbow, shoulder), shoulder shortening. Often, due to severe pain, the patient cannot move the injured arm, so he is forced to keep it with his healthy one.The pain that develops during a fracture is usually much stronger than the pain caused by a bruise. However, unlike a fracture, with a bruise the function of the joint is rarely significantly impaired, and pathological mobility, shortening of the shoulder and crepitus should not occur at all.
The problem is that the patient has these signs ( crepitus, pathological mobility) cannot always be identified independently, due to the existence various types closed fractures of these bones. Therefore, if there is severe pain in the shoulder or elbow joint that occurs immediately after a shoulder injury, all patients should definitely consult a doctor.
Dislocation of shoulder, collarbone
A dislocation is a pathological situation in which the bones that connect to each other become separated in the joints. With shoulder bruises, dislocations of the shoulder or collarbone are quite common. They are observed when patients fall on the elbow, shoulder, or direct blows to the area of the shoulder or acromioclavicular joints. With these dislocations, patients complain of sharp local pain in the area of the damaged joint, its swelling, and shoulder deformity. If the shoulder joint is dislocated, the patient also makes additional complaints about the inability to carry out any movements in this joint. When a shoulder or collarbone is dislocated, the injured arm is supported by the healthy arm. Painful sensations with such dislocations they are caused by damage to the joint capsule, cartilage, rupture of ligaments, damage to the periosteum, and compression of nearby nerves and vessels.Muscle inflammation
When a shoulder is bruised, not only the skin and subcutaneous fat tissue are injured and inflamed, but sometimes also skeletal muscles. Inflammation of skeletal muscles ( myositis) develops for the same reason as the bruise itself ( due to mechanical trauma), therefore myositis quite often accompanies bruises. Inflammation of muscles during bruises is usually limited to the site of injury; it does not spread to adjacent tissues. With myositis in the damaged area of the shoulder, muscle pain and swelling occurs in the muscles, mobility in the joints is limited ( due to pain in the muscles that regulate movement in it). Painful sensations during myositis intensify with the slightest involvement of the affected muscles in movements, as well as with palpation of the bruise site.Sprain
A sprain is a situation in which part of the connective tissue fibers are torn. Since ligaments are a component of the articular apparatus, sprains are usually observed in the joint area ( shoulder or elbow) shoulder region. Sprains often accompany bone fractures and dislocations, which can occur with shoulder injuries. When there are only shoulder contusions, sprains are less common.Distinguish simple stretching ( that is, a sprain that developed independently, without a fracture or dislocation) from a shoulder bruise that occurs after injuries to the shoulder area is practically impossible, since they clinical symptoms very similar. With a sprain, just like with a bruise, pain, bruising, swelling at the site of injury, and limited mobility of the affected joint may occur.
Inflammation of the shoulder or elbow joint
Shoulder bruises can damage the joints ( elbow or shoulder). If their tissue is damaged ( articular cartilage, periosteum, articular capsule, etc.) become inflamed, causing the joint to increase in size and pathological fluid to accumulate in it. If the joints are severely damaged, small vessels may rupture, causing blood to accumulate in the joint cavity. This condition is called hemarthrosis. The appearance of hemarthrosis and the accumulation of pathological fluid in the joint cavity, as well as inflammation in its tissues, lead to a significant limitation of articular movements in the affected joints and the occurrence of intense pain.Tendon damage
Shoulder bruises, which are complicated by dislocations, are often combined with ruptures of muscle tendons. The most common type of injury that occurs is a torn rotator cuff tendon. This cuff is a combination of several muscles ( infraspinatus, supraspinatus, subscapularis, teres minor) the shoulder girdle of the upper limb and their tendon bundles attached to the head of the humerus. The muscles that make up the rotator cuff are essential for strengthening and stabilizing the position of the humeral head in the shoulder joint. They are involved in abduction, adduction and rotational joint movements in the shoulder joint.When the tendons of these muscles rupture, movement in the shoulder joint becomes impaired. It causes pain and discomfort. Pain syndrome ( characteristic of rotator cuff tendon rupture) is often disguised as intense pain that develops as a result of dislocation and bruise. Therefore, such a gap often cannot be detected in the early stages. It is usually diagnosed after the dislocation has been treated. As a rule, in patients who have suffered a shoulder dislocation, pain and discomfort in the shoulder area do not go away completely. This forces them to again seek help from their doctor, who, after conducting additional tests, may identify a rupture of the rotator cuff tendons.
Peripheral nerve damage
For uncomplicated shoulder injuries ( no fractures, dislocations, etc.) minor damage to the peripheral nerves of the arm may occur. Most often, such injuries are manifested by pain, short-term numbness of the limb, tingling sensation, impaired motor ( motor) functions of certain muscles, redness or paleness of the skin on the shoulder. If a shoulder bruise occurs simultaneously with a fracture or dislocation, the damage to the nerves can be very significant ( muscle paralysis, persistent disorders of skin sensitivity, dysregulation of vascular tone, etc.).In severe shoulder injuries, the most commonly injured nerves are the axillary, subscapularis, ulnar, musculocutaneous, and radial nerves. The first two nerves, for example, are often damaged by bruises accompanied by shoulder dislocations or fractures of the head of the humerus. Their damage is characterized by loss of skin sensitivity on the upper lateral ( external side) surface of the shoulder and paresis ( decreased muscle strength) supraspinatus, infraspinatus ( subscapular nerve), teres minor, deltoid muscles ( axle), resulting in impaired supination ( outward rotation) and shoulder abduction.
Defeat radial nerve may be accompanied by impaired skin sensitivity on the posterior surface of the shoulder, forearm and radial ( ray) surface of the hand, as well as paresis ( decreased muscle strength) triceps brachii and wrist extensor muscles. Due to such paresis, the hand will not be able to extend at the wrist, and the forearm at the elbow joint. Damage to this nerve usually occurs with shoulder bruises, complicated by closed fractures of the humerus in the area of its diaphysis ( middle part of the bone), lower metaphysis or epiphysis ( lower part of the bone).
When the musculocutaneous nerve is injured, paralysis occurs ( ) biceps, brachialis and coracobrachialis muscles, the sensitivity of the skin on the lateral ( external side) side of the forearm. Due to such an injury, muscle weakness develops when the forearm is rotated outward and flexed at the elbow joint.
When the humerus is fractured in the area of its condyle, damage to the ulnar nerve often occurs. It is accompanied by impaired sensitivity of the skin on the elbow ( inner side) side of the forearm, hand and fingers ( in the area of III, IV, V fingers). The fingers of the hand lose the ability to perform various movements - adduction, flexion, extension, extension, etc.
Open shoulder injuries
A shoulder bruise is often combined with bruised wounds. These wounds appear as a result of a blow to the shoulder area with a blunt object ( bottle, stick, metal rod, etc.). The edges of bruised wounds are always blurred, bleeding from them is very weak or absent altogether ( since they mainly destroy small superficial vessels, which immediately thrombose). There is pain and swelling at the site of injury. If the injury occurs in the joint area ( elbow, shoulder), then their function is partially disrupted.With more serious types open shoulder injuries ( chopped, crushed, gunshot) there is unbearable pain, swelling and deformation of the shoulder, severe bleeding from the wound, the integrity of the superficial ( skin, subcutaneous fat) and deep tissues ( muscles, ligaments, tendons, bones, nerves, blood vessels), and with it the various functions of the hand.
What to do if you hit your shoulder hard?
For such bruises, it is recommended to take anti-inflammatory drugs ( , dexalgin, etc.). There is no need to call an ambulance in such cases. However, it is still worth going to the emergency room for a consultation with a traumatologist so that he can check the safety of deeper anatomical formations ( ligaments, bones, joints).
Exactly the same first aid is provided if a shoulder bruise occurs in the area of the shoulder or elbow joints of the arm. In these cases, the pressure bandage does not need to be applied to the affected joint. Also, to reduce pain, it is recommended to move and feel the bruised area on the arm less. If you have a joint injury, you must go to the trauma department. Since, in most cases, with such injuries, pathological fluid accumulates in the cavity of the damaged joints, which must be removed using joint puncture.
If, after a strong blow to the shoulder, a complicated bruise of the shoulder appears, then in this case you need to act based on the situation. When a shoulder bruise is combined with a superficial wound, it must be treated with some kind of antiseptic ( alcohol, brilliant green) and apply a sterile bandage on top. After that, apply cold to the site of the injury and use an anesthetic. Then you need to go to the emergency room.
- with a fracture ( open and closed) or dislocation of arm bones;
- with impaired sensitivity of the skin of the hand ( shoulder, forearm, hand);
- with paresis ( weakening of muscle strength) or paralysis ( loss of muscle contractility) arm muscles;
- with polytrauma ( that is, simultaneous injury to the shoulder and other anatomical areas of the body);
- with impaired vascular patency ( whitening and coldness of the limbs);
- with massive damage to the tissues of the arm, which occurs with chopped, crushed, gunshot wounds of the shoulder.
In the presence of bruises with massive damage to the tissues of the shoulder, accompanied by intense arterial bleeding from the wound, the primary task is to temporarily stop it. It can be done on a short time using finger pressure on the brachial artery above the wound site on the shoulder. This artery passes through the medial ( inner side) side of the shoulder and is adjacent to the humerus there; it can be easily found there by the sensation of rhythmic pulsating movements. The brachial artery must be pressed against the humerus. Finger pressure can be used for minor bleeding, as well as in the intermediate period between searching and applying a tourniquet.
Application of a tourniquet is a longer and reliable method stops arterial bleeding. For bleeding from the shoulder area, a tourniquet is also applied above the bleeding site. It is best tied along the humerus, although in some cases it can also be placed in the armpit for high shoulder injuries.
When applying a tourniquet, you should know the following basic rules:
- a tourniquet is applied above the bleeding site and as close to it as possible;
- Before installing the tourniquet, you need to place it in the place where it will be applied. soft tissue;
- when tying a tourniquet, it is necessary to lift the affected limb upward;
- Be sure to check the reliability after applying the tourniquet ( absence of pulse in the brachial artery located below the site of bleeding, cessation of bleeding from the wound, paleness and coldness of the arm below the site of injury);
- after installing the tourniquet, it is necessary to record the exact time of its application;
- Every hour after applying the tourniquet, it must be loosened for 10 to 15 minutes ( to avoid premature necrosis of hand tissues).
For shoulder bruises combined with closed fractures of the humerus and joint dislocations ( acromioclavicular or brachial) the first step is to immobilize ( immobilize) injured hand.
Immobilization for humerus fractures is carried out using a Cramer scalene splint. You can also use dense materials at hand as a splint ( stick, board, umbrella, ski, etc.), which will be slightly longer than the shoulder itself. The splint on the shoulder is strengthened with a bandage ( if it is not available, any long durable fabric will do). With him ( bandage) When applying, the fracture site itself should be avoided.
After strengthening the splint, the injured arm is bent at the elbow at a right angle and suspended by the wrist to the neck. In this case, it is recommended not to use a basket-shaped scarf ( with it, the lower part of the bandage covers almost the entire forearm), since when it is applied, the lower fragment of the humerus will rest against it, which can provoke additional displacement and cause various complications ( damage to blood vessels, nerves, etc.) at the fracture site.
For dislocations of the clavicle and shoulder, immobilization ( immobilization) of the injured limb is done by hanging the arm from the neck using a regular scarf. After immobilizing the arm for shoulder bruises combined with closed fractures of the humerus or joint dislocations, you need to take painkillers and anti-inflammatory drugs ( , ibuprofen, aspirin, etc.). Then you need to go to the traumatology department.
For open fractures of the shoulder, before immobilization, you should first stop the bleeding, if any, and then apply ( not tight) several tampons and a sterile bandage on the wound. The technique for immobilizing the affected limb for such fractures is exactly the same as for closed fractures of the humerus.
It is worth remembering that in case of severe bruises of the shoulder, it is strictly not recommended to try to check the shoulder for the presence of closed injuries ( fractures, dislocations). Also, you should not wait for recovery at home and hope that perhaps everything turned out okay and that no more serious damage to the tissues of the arm other than a simple bruise occurred at the time of the injury. In case of obvious complications ( open fracture, dislocation) do not put your fingers into the wound ( this will lead to tissue infection), make any movements with the damaged joint ( may cause compression of nearby vessels and nerves).
For bruises of the shoulder, accompanied by whiteness and coldness of the hand ( that is, the presence of acute arterial obstruction), victims should be immediately taken to hospital ( to the surgical or trauma department). Before the patient reaches medical institution he is given antispasmodics ( vasodilators), disaggregants ( interfere with the ability to adhere to each other), anticoagulants ( substances that prevent blood clotting and formation in blood vessels). In this case, a pressure bandage and cold are not applied to the affected arm.
If in the arm area ( shoulder, forearm, hand) after a shoulder injury, a violation of skin sensitivity or paresis occurred ( muscle dysfunction) her muscles, then you need to seek help as soon as possible medical care to the traumatology department.
With polytrauma ( that is, simultaneous injury to the shoulder and other anatomical areas of the body) first aid is provided whenever possible. First of all, it is necessary to prevent dangerous conditions, such as stopping the functioning of the respiratory system ( examination of the upper respiratory tract for the presence of foreign bodies, artificial respiration, conicotomy), hearts ( heart massage), blood loss ( tourniquet application). In this case, a shoulder bruise fades into the background. Its treatment should be started after the function of the main organs returns to normal.
Diagnosis of injuries due to a shoulder injury
 Diagnosing the presence of a shoulder injury is quite simple based on the presence of characteristic symptoms ( pain, shoulder dysfunction) and external manifestations ( swelling, the appearance of intradermal and subcutaneous bleeding). This can be done either by the patient himself or by a traumatologist to whom he can turn for help. The problem is that a strong blow to the shoulder area does not always result in only a shoulder bruise. Quite often in these cases, deeper tissues are affected. This is why a traumatologist sometimes performs ( clinical research methods) and assigns some additional diagnostic procedures (radiation, laboratory tests).
Diagnosing the presence of a shoulder injury is quite simple based on the presence of characteristic symptoms ( pain, shoulder dysfunction) and external manifestations ( swelling, the appearance of intradermal and subcutaneous bleeding). This can be done either by the patient himself or by a traumatologist to whom he can turn for help. The problem is that a strong blow to the shoulder area does not always result in only a shoulder bruise. Quite often in these cases, deeper tissues are affected. This is why a traumatologist sometimes performs ( clinical research methods) and assigns some additional diagnostic procedures (radiation, laboratory tests).For diagnosing shoulder contusions(as well as their complications)The following types of studies may be prescribed:
- clinical examination methods;
- radiation examination methods;
- laboratory examination methods;
- additional examination methods.
Clinical examination methods
Clinical research methods allow the doctor to obtain information about the symptoms that are bothering the patient ( the presence of pain, swelling, wounds, dysfunction of the joint in the area of the bruise) and find out from him how and under what circumstances the shoulder injury occurred. These methods are mandatory and necessary either for further planning and assignment of the following diagnostic studies, or to select a treatment method. As a rule, with simple and uncomplicated shoulder bruises diagnostic measures ends with these studies.Clinical examination methods used for shoulder contusions
| Method name | The essence of the method | |
| Anamnesis | The doctor asks the patient about the reasons that prompted the patient to seek medical help, as well as about the conditions ( time, place, mechanism, etc.) in which a shoulder injury occurred. |
|
| Visual inspection | During the interview, the traumatologist pays attention to general state patient, determines the color of the skin, the presence of mobility in the injured limb, the presence open wounds, hematomas, bruises on the skin. |
|
| Palpation | Using his fingers, the traumatologist slowly and carefully feels the site of injury and tactilely determines the place of maximum pain and swelling. He also tries to determine which anatomical structures ( skin, muscles, bones, joint formations) suffered the most damage from a shoulder injury. |
|
If, during a clinical examination of the patient, the attending physician suspects that the victim has any additional damage in addition to the shoulder bruise ( fracture, dislocation, vascular obstruction, joint inflammation, nerve damage, etc.), then he can assign him the passage of radiation ( , and etc.), laboratory ( analysis of blood, joint fluid, etc.) and other studies.
Radiation examination methods
Radiation diagnostic methods can show anatomical structure internal tissues of the body. Therefore, they are often used in clinical practice to detect tissue damage that is located deeper than the skin ( which the doctor examines during an external examination) – muscles, bones, joints, arteries, nerves. Radiation methods are the main ones in diagnosing shoulder injuries and it is with their help, in most cases, that a traumatologist can make a final diagnosis.Radiation examination methods used to diagnose bruises and related complications
| Method name | The essence of the method | What can this method reveal in case of a shoulder injury? |
| X-ray examination | The damaged area of the shoulder is irradiated using X-rays. Having passed through the tissues of the hand, this radiation forms an image on the film that displays the structure of its internal tissues. |
|
| CT scan | ||
| Magnetic resonance imaging | Patient's body ( along with an injured shoulder), passing through a magnetic resonance imaging scanner, is exposed to electromagnetic waves of a certain frequency. These waves cause excitation of atoms in tissues, which is recorded by the scanner of this device. This method is the most accurate and allows you to identify even the most insignificant pathological changes inside tissues that cannot be detected CT scan and radiographic examination. | |
| Ultrasonography | The bruised area is illuminated with ultrasonic waves. Ultrasound cannot be used in diagnosing fractures, since bone tissue pushes away ( due to its density) ultrasonic waves. |
|
| Angiography | A traumatologist injects a contrast agent into the damaged vessels of the patient’s shoulder. Then, using radiation research methods ( radiography, computed tomography,) watches how it will be distributed among them. |
|
| Arthrography | A liquid contrast agent is injected into the joint cavity, and then an x-ray is taken, which depicts the distribution of this substance within the joint. |
|
| Arthroscopy | Into a joint damaged by a bruise ( shoulder, elbow) a special probe equipped with a video camera is inserted. Using this probe, the joint cavity is examined for any changes. |
|
Laboratory examination methods
Laboratory methods examinations are not always necessary when diagnosing shoulder injuries. They are most often used for joint damage ( synovial fluid examination), open fractures of the humerus, accompanied by intense bleeding ( And). Also their ( microbiological analysis) can be prescribed for bruises of the shoulder, accompanied by open wounds of this area and infection of the superficial ( skin, muscles) or deep ( joints, bones) hand tissues.Laboratory tests that are prescribed for shoulder bruises
| Method name | The essence of the method | What can this method reveal in case of a shoulder injury? |
| General analysis blood | Using a syringe or special vacuum tubes, several milliliters of blood are taken from the victim’s cubital vein. Next, she is taken to the laboratory for her general ( determine the number of cells, hematocrit, etc.) or biochemical research (determine the presence of inflammatory substances, minerals, etc.). |
|
| Biochemical analysis blood |
|
|
| Synovial fluid examination | To obtain synovial ( articular) liquid, a traumatologist performs a puncture of the joint damaged by a bruise. After which he sends her to a laboratory that studies the various components of this liquid ( cellular, biochemical, microbiological). |
|
Additional examination methods
From additional methods examinations that can be used in diagnosing bruise injuries include joint puncture and electromyography.Joint puncture is a procedure in which the joint cavity ( for example, shoulder or elbow) a needle is inserted through which the joint fluid is sucked out using a syringe. This procedure is often used for shoulder bruises that occur in the joint area and are accompanied by the accumulation of pathological fluid ( effusion, blood) in their cavity. Often, a traumatologist can send the fluid obtained during puncture to the laboratory, where it will be further examined and provide him with information about the nature of the pathological processes occurring inside the joint.
Electromyography is a research method that records electrical impulses that occur when skeletal muscles are excited. This study sometimes performed for myositis ( muscle inflammation), availability muscle weakness, intense muscle pain or damage to peripheral nerves.
The essence of this method is that at the site of injury on the shoulder ( or in any other area of the arm where there is disruption of normal muscle function) several electrodes are applied and connected to a device - an electromyograph. It registers bioelectric impulses coming from the affected muscles to the electrodes. If a muscle is damaged or its innervation is disrupted, research results will indicate that its electrical excitability will be reduced ( decrease in the amplitude and frequency of electrical oscillations on the electromyogram - a graphic image obtained during electromyography).
Shoulder sprain
 When the ligaments of the shoulder joint are sprained, a slight disruption of their microstructure and function occurs, due to which part of the connective fibers that make up these ligaments is partially torn. The entire shape and structure of the ligaments themselves remains unchanged. However, the ligaments in these cases often thicken due to inflammatory processes that develop in them after stretching their connective tissue fibers. This actually distinguishes a rupture of the ligaments of the shoulder joint from a simple sprain.
When the ligaments of the shoulder joint are sprained, a slight disruption of their microstructure and function occurs, due to which part of the connective fibers that make up these ligaments is partially torn. The entire shape and structure of the ligaments themselves remains unchanged. However, the ligaments in these cases often thicken due to inflammatory processes that develop in them after stretching their connective tissue fibers. This actually distinguishes a rupture of the ligaments of the shoulder joint from a simple sprain. Sprains of the shoulder joint can occur when the shoulder is bruised, when performing various physical exercises that exceed the range of motion in the shoulder joint, as well as when lifting heavy objects. This injury often occurs in athletes who do not spend enough time warming up. physical exercise in the shoulder joint, before major sports exercises.
The following symptoms are typical for a sprained shoulder joint:
- pain in the shoulder joint;
- swelling at the site of injury;
- redness of the skin covering the shoulder joint;
- discomfort in the shoulder joint;
- increase in size of the shoulder joint;
- limited mobility of the shoulder joint;
- bruising;
- increased pain upon palpation of the shoulder joint.
What structures are inflamed during stretching?
When sprained, connective tissue fibers, which are the main component of ligaments, are mainly injured. When the ligaments of the shoulder joint are sprained, other joint structures are often damaged along with them - cartilage, joint capsule, joint capsules ( subscapularis, subcoracoid, etc.). With bruises of the shoulder joint, the process may involve the periosteum, muscles, muscle tendons, subcutaneous fat, and skin.Which doctor should I contact if I have a sprain?
If you have injuries to the shoulder joint, you should consult a traumatologist or surgeon. Athletes usually consult a sports doctor. After clinical examination ( collection of anamnestic data, external examination, palpation) these doctors can prescribe a patient to undergo additional research (ultrasonography, radiography, magnetic resonance imaging, etc.) to confirm the diagnosis of shoulder sprain.Is it possible to treat sprains at home?
With a simple sprain of the shoulder joint, treatment is carried out at home, since such injuries do not pose any serious threat to patients. Sprains of the shoulder joint, which occur as a result of fractures, dislocations, and severe bruises of the shoulder, are treated both on an outpatient basis and in the hospital. It all depends on the severity of the damage. Moreover, the main treatment, as such, in such cases is more aimed at eliminating more serious pathology ( fracture, dislocation) rather than the stretch itself. This is due to the fact that ligaments have a great regenerative capacity and can themselves restore their anatomical structure, except in cases of complete rupture. Torn shoulder ligaments are treated surgically.How to treat sprains at home?
Immediately after a sprain, you need to apply something cold to the injury site ( ice bag, cold water ). Cold is applied to the site of injury not directly, but through some tissue. The duration of cold application should be no more than 1 – 2 hours. After this, it is recommended to immobilize the shoulder using a scarf bandage, which can be hung from the victim’s neck. After placing the injured arm in such a bandage, you should wait another 20–30 minutes, and then again apply cold to the injury site for 1–2 hours. Such alternations ( application and removal of cold) can be repeated for 1 – 2 days from the moment of injury. In addition to immobilizing the shoulder joint with a scarf, you must also strictly ensure that you do not make any movements in the shoulder joint. This is one of the main principles of successful treatment of sprains.For shoulder sprains, it is recommended ( especially with severe pain syndrome ) the first few days periodically use ( ibuprofen, aspirin, etc.). This will help reduce pain and swelling at the injury site. If the injury does not cause the victim significant discomfort, pain or other symptoms, then these medications do not need to be used.
After the main discomfort has passed ( pain, swelling, discomfort) at the site of injury, it is necessary to gradually begin to make slight movements in the shoulder joint. This should be done slowly and gradually, increasing the range of motion, as well as increasing the mechanical load on the shoulder joint. Recovery movements after a sprain should always be performed, otherwise a relapse may occur ( re-stretching) injuries.
Such a simple and affordable treatment for sprained shoulder joints is due to its pathogenetic nature ( that is, focusing on the pathological mechanism) methods used. Cold and anti-inflammatory drugs help reduce inflammation in damaged ligaments, immobilization and lack of movement speed up regeneration processes ( recovery) tendons, rehabilitation exercises - strengthen the restored ligaments.
Damage to the shoulder muscles ( myositis)
 Myositis is pathological process, in which inflammation of skeletal muscles located in any part of the human body occurs. With a simple bruise of the shoulder, such inflammation is caused by a minor mechanical shock and partial destruction of muscle fibers. In case of shoulder bruises accompanied by open injuries, the cause of myositis can be various microorganisms that penetrate the muscle tissue through the wound surface. Myositis can also be caused by congenital or autoimmune pathology, intoxication with chemicals, physical overload, viral infection and etc.
Myositis is pathological process, in which inflammation of skeletal muscles located in any part of the human body occurs. With a simple bruise of the shoulder, such inflammation is caused by a minor mechanical shock and partial destruction of muscle fibers. In case of shoulder bruises accompanied by open injuries, the cause of myositis can be various microorganisms that penetrate the muscle tissue through the wound surface. Myositis can also be caused by congenital or autoimmune pathology, intoxication with chemicals, physical overload, viral infection and etc. The following symptoms usually indicate the presence of shoulder muscle myositis:
- shoulder muscle pain ( may be at rest or appear when moving the arm, or when pressing on the muscles);
- muscle swelling;
- weakness in the shoulder muscles;
- limited mobility in the joint ( shoulder or elbow);
- decreased muscle endurance;
- amyotrophy ( that is, a decrease in muscle volume and mass);
- decreased ability to work in the injured arm.
What structures are inflamed during myositis?
With myositis, muscles become inflamed and connective tissue. If myositis is a consequence of a shoulder injury, then the tissue adjacent to the muscles - subcutaneous fat, blood vessels, nerves, skin, periosteum - can also be damaged at the site of inflammation.Which doctor should I contact for myositis?
The diagnosis and treatment of traumatic myositis is carried out by a traumatologist. If, when a patient contacts this doctor, it turns out that myositis is not of traumatic etiology ( origin), then he will most likely be referred for consultation to a rheumatologist ( if the traumatologist suspects that muscle inflammation is caused by a genetic or autoimmune pathology) or infectious disease specialist ( if the traumatologist suspects an infectious origin of myositis).Diagnosis of myositis
The presence of simple traumatic myositis can be determined by a traumatologist immediately after a clinical examination of the patient. This type of myositis occurs directly at the site of injury and its symptoms are similar to a shoulder bruise. However, when communicating the diagnosis to the patient, the attending physician tells him that the suspected injury is a simple shoulder contusion and not traumatic myositis. This is done because with shoulder bruises there is no limited muscle damage without damage to more superficial tissues ( skin, subcutaneous fat).Dislocation of the shoulder joint can be observed when falling on an outstretched arm, on the shoulder, on the elbow, with direct blows to the shoulder area, compression of the torso, etc. Depending on the direction of displacement of the head of the humerus relative to the articular surface of the scapula, anterior, posterior and inferior dislocations of the humerus are distinguished . The most common are anterior shoulder dislocations ( occur in 97 – 98% of cases). They, in turn, are divided into subclavian, subcoracoid and intracoracoid types.
With subclavian dislocation, the head of the humerus is displaced medially ( inner side) side and is located directly under the collarbone. In a subcoracoid shoulder dislocation, the head of the shoulder is located directly under the coracoid process. If the head of the humerus is half or less under the coracoid process, then such dislocations are called intracoracoid.
The presence of a shoulder dislocation is confirmed by the following symptoms:
- sharp pain in the shoulder area;
- lack of active articular movements in the shoulder joint;
- shoulder joint deformity;
- forced position ( the patient supports the injured arm with his healthy arm, which he bends at the elbow and slightly moves away from the body, while his head is tilted towards the injured arm) bodies;
- lengthening of the injured shoulder;
- the elbow on the affected side cannot be brought to the body;
- the presence of springy passive movements in the shoulder joint;
- the presence of tension in the muscles surrounding the shoulder joint.
What structures are damaged during dislocation?
When a dislocation occurs, the articular cartilage of the head of the humerus and the glenoid cavity of the scapula are damaged. Also, with such a dislocation, rupture and damage to the joint capsule, ligaments, joint capsules, tendons, and muscles often occurs. In some cases, such an injury is complicated by mechanical compression of blood vessels, nerves, intra-articular bone fracture, and injury to the periosteum.Which doctor should I contact if I have a dislocation?
A traumatologist diagnoses and treats dislocations. Before contacting this specialist, you can call an ambulance, whose staff will provide all the necessary measures to immobilize and transport the victim to the traumatology department.Is it possible to treat a dislocation at home?
If a dislocation occurs at home, only first aid can be provided to the patient. It consists of immobilization ( immobilization) injured arm using a scarf bandage, taking painkillers ( analgin, ibuprofen, aspirin, etc.) and transporting the patient to the traumatology department. You don't need to do anything else yourself. This is especially true for manually reducing dislocations, which should under no circumstances be performed, because it can lead to serious consequences.Doctors often perform the reduction of fresh simple and uncomplicated dislocations on an outpatient basis, without hospitalizing the patient. That is, after reducing the dislocation, the traumatologist can immediately send the patient home, having first immobilized the reduced joint with a plaster cast. In the presence of serious, complicated dislocations, they usually resort to inpatient treatment (hospital treatment).
How is a dislocation treated at home?
After the traumatologist has put a plaster cast on the patient in the hospital, he can be sent home. At home, treatment for a dislocated shoulder is that the patient needs to provide complete rest to the injured arm and monitor his own condition ( to quickly identify complications). In some cases, the doctor may prescribe painkillers or anti-inflammatory drugs. After removing the plaster ( on average, the immobilization period ranges from 3 to 5 weeks) the patient must carry out therapeutic exercises, undergo a massage, and monitor the load on the shoulder joint. The duration of the recovery period is usually 2 – 3 weeks.
What folk remedies are used to treat shoulder bruises?
 Most of the famous folk remedies treatment of shoulder bruises has an anti-inflammatory and analgesic effect, which is why their use is so widespread. However, do not forget that with shoulder bruises, certain complications may arise ( closed fracture, rupture of ligaments, tendons), which can only be cured with medication and surgical methods treatment. Therefore, after a shoulder injury occurs, it is first recommended to consult a traumatologist so that he can rule out various complications and diagnose the presence of a simple bruise. This doctor may also advise you to choose a more effective method treatment with drugs.
Most of the famous folk remedies treatment of shoulder bruises has an anti-inflammatory and analgesic effect, which is why their use is so widespread. However, do not forget that with shoulder bruises, certain complications may arise ( closed fracture, rupture of ligaments, tendons), which can only be cured with medication and surgical methods treatment. Therefore, after a shoulder injury occurs, it is first recommended to consult a traumatologist so that he can rule out various complications and diagnose the presence of a simple bruise. This doctor may also advise you to choose a more effective method treatment with drugs. For a shoulder injury, you can use the following folk remedies:
- Potato compresses. Take a few raw potatoes and grate them. Then make a compress from the resulting porridge. It should be applied to the site of a shoulder bruise 3 to 4 times a day for 30 minutes.
- Horsetail infusion. Take 50 g of horsetail herb and add it to a container filled with 0.5 liters of boiling water. Then the resulting mixture must be infused for 30 - 40 minutes. Next, you need to make compresses from the horsetail tincture, which are applied to the damaged area of the shoulder 2–4 times a day.
- Arnica flower tincture. Add 5 g of arnica flowers to one glass of boiling water. Infuse and filter. Then use this tincture in the form of compresses, which are applied to the site of the bruise ( for 30 – 60 min) 3 – 4 times a day.
- Sophora tincture. Place half a glass of Sophora fruits in one glass of vodka. Then this mixture must be infused and filtered. Tincture of Sophora fruits should be taken 3-5 times a day, 10 drops.
- Tincture of hyssop. In order to make such an infusion, you need 20 g of medicinal hyssop, which is diluted in one glass of vodka. Then this mixture must be infused for 7 - 8 days. This tincture is taken orally, one tablespoon 2 - 3 times a day, 20 - 30 minutes before meals.
What ointments can be used for a shoulder injury?
 Painkillers for a shoulder injury can be used not only in tablet forms, but also in the form of ointments ( or gels, sprays, etc.). Use of such dosage forms significantly accelerates the effect of the main active components included in the preparations. Ointments are more effective and have a less toxic effect on the body compared to tablets.
Painkillers for a shoulder injury can be used not only in tablet forms, but also in the form of ointments ( or gels, sprays, etc.). Use of such dosage forms significantly accelerates the effect of the main active components included in the preparations. Ointments are more effective and have a less toxic effect on the body compared to tablets. When a shoulder is bruised, non-steroidal anti-inflammatory ointments, local irritants, and local anesthetics can be applied to the damaged tissues ( painkillers). The first drugs, penetrating into damaged tissues, block the formation of an enzyme in them - cyclooxygenase, which promotes the release of inflammatory substances from them ( prostaglandins, leukotrienes, prostacyclins, etc.). Thus, non-steroidal anti-inflammatory substances reduce inflammatory reactions at the site of injury, which reduces pain, swelling, and redness of tissues.
Local irritants have a local irritant effect on the skin by stimulating its nerve endings. This irritation leads to dilation of the superficial vessels of the skin, increasing their blood supply and resorption ( resorption) necrotic tissues. These agents are stimulants of regeneration ( recovery) surface covers. Local irritants cannot be used immediately after a bruise, since in the first days of a bruise, cooling and anti-inflammatory therapy is strictly indicated ( use of cold, anti-inflammatory substances). All local irritants are divided into warming and cooling.
When using warming ointments, a feeling of warmth immediately appears at the site of injury, pain, discomfort and swelling are reduced. These ointments are usually applied to the site of injury during rehabilitation ( restorative) period, as well as with some complications of bruises ( inflammation of muscles, ligaments, tendons, joints, etc.).
Cooling ointments have a less pronounced irritating effect than warming ones. When applied to the skin, these ointments cause a cooling effect, but despite this, they do not provoke a decrease in its temperature, but, on the contrary, raise it slightly. Cooling ointments are often used in the treatment of shoulder bruises. They are usually prescribed on days 2–6 from the moment of injury. It all depends on its seriousness.
Local anesthetics cause a temporary loss of sensation in the damaged tissue, which is why the patient does not feel pain at the site of the shoulder injury. These drugs do not help reduce inflammation in bruised tissues, so you should not overuse them.
Ointments used for shoulder bruises
| Drug group | Drug name | Method of application |
| Nonsteroidal anti-inflammatory drugs | Diclofenac | It is necessary to apply to the site of injury 2–4 times a day. Each time you need to use 2 - 4 grams of ointment. It is recommended to wash your hands every time after rubbing in the medicinal product. |
| Ibuprofen | Apply 2–5 g of ointment to the site of injury 2–4 times a day. | |
| Indomethacin | For shoulder bruises, this ointment should be applied a few grams 3 to 4 times a day. | |
| Ketoprofen | This ointment is rubbed over the bruise 2-4 times a day. | |
| Local anesthetics
(painkillers) | Menovazin | The ointment is rubbed into the bruised area 2 - 3 times a day. |
| Local irritants
(cooling ointments) | Bom Benguet | Apply 2 - 4 g of this ointment to the bruise on the shoulder 1 - 3 times a day. It can be used for no more than 10 days without consulting your doctor. |
| Gevkamen | This ointment must be applied in a thin layer 2 to 3 times a day. | |
| Efkamon | Apply 2–3 grams of ointment to the site of injury two or three times a day. | |
| Local irritants
(warming ointments) | Nicoflex | The ointment should be applied in a thin layer to the site of the bruise 1 – 2 times a day. |
| Finalgon | The drug can be applied to the site of injury 1 – 3 times a day. Moreover, the length of the ointment column when applied once should be no more than 0.5 - 1 cm per skin area equal to 20 cm 2. | |
| Viprosal | You need to apply 5 - 10 grams 1 - 2 times a day. |
What to do if you can’t raise your arm after a shoulder injury?
 Some shoulder injuries can have serious complications. One of them is a complete impairment of mobility in the shoulder joint, which disrupts movement in the entire arm. The main causes of this pathology may be a dislocated shoulder, a fracture of the humerus, or damage to the brachial plexus.
Some shoulder injuries can have serious complications. One of them is a complete impairment of mobility in the shoulder joint, which disrupts movement in the entire arm. The main causes of this pathology may be a dislocated shoulder, a fracture of the humerus, or damage to the brachial plexus. When the shoulder is dislocated, the head of the humerus comes out of its articulation with the scapula. This results in the muscles that control the shoulder joint being unable to move in any direction. humerus, which leads to impaired mobility of the entire arm. Some fractures of the humerus may be accompanied by dislocations of the shoulder or lead to partial destruction of the articular surface of the head of the humerus. The consequences of such fractures are the same as with a dislocated shoulder.
Severe shoulder contusions may be associated with significant injury to the brachial plexus. From this plexus emerge all the nerves that innervate the tissues of the upper limb, including muscles. Damage to the brachial plexus may be accompanied by complete or partial paralysis of the muscles of the arm, due to which the patient will not be able to perform any active actions ( raise, lower, rotate, adduct, abduct the arm, etc.).
You can distinguish a brachial plexus injury from a shoulder dislocation or humerus fracture by the prevalence of symptoms. In case of damage to the brachial plexus, skin sensitivity throughout the entire arm most often disappears, and the ability to move the muscles of the shoulder, forearm, and hand occurs. Pain may be localized below or above the shoulder. In case of dislocation or fracture, symptoms ( pain, swelling, bruising, limited mobility in joints, etc.), usually limited to the shoulder region ( but not always, since these injuries can damage nerves and blood vessels). In any case, only a doctor can confirm the presence of a particular injury by conducting a clinical examination ( anamnesis, external examination, palpation) and radial ( radiography, computed tomography, etc.) examination of the patient.
All three ailments are quite serious pathologies, so they can only be treated in a medical institution ( in the trauma department). If, after a shoulder injury, the victim cannot raise his arm ( or do another active action) she needs to be immobilized ( immobilize) before seeking help at the emergency room. This must be done to ensure that the patient does not experience additional complications during transportation.
In order to immobilize the injured limb ( for dislocations and injuries of the brachial plexus), you must first bend it at the elbow joint, bring it towards the body and hang it by a scarf covering most of the forearm. For fractures of the humerus, the arm should be suspended only by the wrist using a narrow and strong bandage. If it is not possible to provide first aid to the victim, you should call an ambulance.
What to do if you bruise your shoulder joint?
 When a shoulder joint is bruised, inflammation of its internal and external structures often develops ( joint capsule, cartilage, ligaments, joint capsules), due to which the patient experiences pain and discomfort in this area, the joint increases in size ( due to swelling of its tissues), physiological mobility is impaired. The skin over the joint turns red and bruises appear. In such cases, it is recommended to immobilize immediately after the injury ( immobilize) hand with a bandage, apply something cold to the joint and take non-steroidal anti-inflammatory drugs ( ibuprofen, etc.). These actions will temporarily relieve the symptoms that bother the victim and prevent possible complications.
When a shoulder joint is bruised, inflammation of its internal and external structures often develops ( joint capsule, cartilage, ligaments, joint capsules), due to which the patient experiences pain and discomfort in this area, the joint increases in size ( due to swelling of its tissues), physiological mobility is impaired. The skin over the joint turns red and bruises appear. In such cases, it is recommended to immobilize immediately after the injury ( immobilize) hand with a bandage, apply something cold to the joint and take non-steroidal anti-inflammatory drugs ( ibuprofen, etc.). These actions will temporarily relieve the symptoms that bother the victim and prevent possible complications. When a shoulder joint is bruised, various complications often occur, such as rupture of the joint capsule, tendons, ligaments, intra-articular bone fracture, shoulder dislocation, hydrarthrosis ( accumulation of pathological fluid in the joint), hemarthrosis ( accumulation of blood in the joint) etc. Therefore, after providing first aid, you should immediately consult with a traumatologist at a medical institution.
SUBSCLATURE MUSCLE manifests itself... when we shiver from the cold. It causes a lot of problems because of its location. Subscapularis muscle is located exactly where its name indicates - under the shoulder blade, more precisely, between the shoulder blade and the chest. Therefore, it is difficult to influence her.
Stand with your arms down so that your palms are touching your outer thighs. Rotate your arm outward so that your palms are facing forward. To rotate your arms to their previous position and turn your palms inward, you need to use the subscapularis muscles.
In the worst case, pain caused by tension points in the subscapularis muscles causes you to slouch, makes it difficult to raise your arms, and limits the movement of your hands. It is usually located just behind the shoulder, at the back of the deltoid muscle, and can be quite severe even when the arm is not in use.
Points of tension in the subscapularis muscles develop in those moments when you have to stop yourself from falling (this happens to any athlete at one time or another). They also develop from movements that require continuous rotation of the arm forward (for example, from the throwing movement). Swimmers, pitchers, tennis players and ball players are often at risk. Stress points in the subscapularis muscle may develop some time after the arm is immobilized in a cast or sling. This means that pain may continue after the injury has healed.
Tension points in this muscle are difficult to find and heal without leaving a trace, but it is possible. Take a position on the bullet in which painful hand hangs between your legs. This allows the sharp outer edge of the shoulder blade to protrude. Thumb Reach under the shoulder blade to find tight cords and a painful point in the muscle that lies on the inner surface of the shoulder blade. Having determined the location of the point, press on it for 15-20 seconds. Then move on to finding another stress point.
Try to find tender spots in the muscle along the outer edge of the shoulder blade, and then reach under it as far as you can to find other spots. Remember that you are trying to reach between the shoulder blade and the rib cage to find the muscle that protects the shoulder blade, and therefore the arm, from moving from chest. It will take work, patience and possibly many sessions before the muscle relaxes. Perform stretching according to certain rules.
Stretch 1: Bend at the waist so that your torso is parallel to the floor and your affected arm hangs freely. Rest your other hand on the table. Take a heavy object in your sore hand. Relax and allow gravity to pull the weight toward the floor, stretching the subscapularis and moving your scapula across your ribcage. Draw a small circle with your hand.
Stretch 2: Place your hands on the doorway. Lengthen your body forward through your outstretched arms, opening your chest and shoulders. First, place your arms so that your elbows are level with your shoulders. Then spread your arms completely, placing your hands above your head (or as high as you can lift them).-
Stretch of the 3rd subscapularis muscle
Stretch 3: bending your arm at the elbow 90°. Raise your affected arm as high as you can. Place your forearm behind your head. Increase the stretch by applying slight back pressure above the elbow.-

Stretch 4: Place your palm on the wall in front of you. Run your fingers up the wall, getting as high as possible, then stand sideways and do the same.
The subscapularis muscle has a wide and thick triangular shape. It runs along the entire costal surface of the scapula. When it is affected by inflammation, pain and other unpleasant symptoms are noted. Let's take a closer look at the function of the subscapularis muscle, as well as how diseases and pathologies associated with it are treated.
Function of the subscapularis muscle
The subscapular region has fleshy areas. With the help of a flat tendon, it is attached to the lesser tubercle and the crest of the lesser tuberosity of the humerus bone.
The subscapularis muscle allows the shoulder to rotate inward while simultaneously bringing the shoulder toward the body. The muscle is innervated by the subscapular nerve, and the blood supply is by the subscapular artery.
Muscle problems and diagnosis
If inflammation develops or other problems arise in the subscapular region(for example, tendon rupture, the appearance of serious diseases), the person feels pain in the shoulder. If you have this symptom, you need to examine:
- muscle tissue;
- all muscles;
- upper limbs;
- shoulder area;
- deltoid muscle;
- supraspinatus and infraspinatus muscles;
- other important muscles, according to the doctor.
The examination is carried out using ultrasound of the muscles, as well as palpation. The doctor orders a blood test for the patient to check the levels of lactic acid, lactate dehydrogenase and total creatine kinase in the blood. If necessary, other diagnostic methods are carried out.
Causes of pain under the shoulder blades
The subscapularis muscle may ache due to scapular-costal syndrome, which is provoked by chest abnormalities, muscle hypertonicity, hypothermia, psycho-emotional trauma and stress. Muscle inflammation and pain can affect the area under both the left and right shoulder blades.
There may be pain under the left shoulder blade due to injuries, incorrect position during sleep, acute respiratory infections or flu, shoulder dislocation, fracture, tear of the rotator cuff, compression of nerves, trigger points, subscapular inflammation, diseases of internal organs.
Under right shoulder blade pain and inflammation occur due to cholecystitis, myocardial infarction, liver disease, breast cancer, shoulder arthritis, biomechanical and other reasons.
Development of tendinopathy
With tendinopathy of the subscapularis muscle, degenerative changes occur. Most often they are provoked by insufficient blood supply to the shoulder muscles or hereditary connective tissue pathology.
The pain with this disease becomes stronger when a person scratches his face, eats with a spoon, or moves his arm behind his back.
Tendopathy of the muscle under the shoulder blade can also occur due to persistent tendon injuries.
Appearance of gaps
Often, if not treated properly, tendinopathy leads to rupture of the subscapularis muscle. When a rupture occurs, a sharp pain is felt. The person cannot move his arm independently.
If the tendons in the subscapular region are partially torn, the victim can move his arm. In cases where the tendon is completely ruptured, the patient is unable to even lift the limb.
The affected subscapular area is fixed with a tight bandage or splint. Once the pain goes away and the shoulder gradually returns to its function, it is recommended to perform exercises to develop the joint.
If the tendon is completely ruptured, the doctor performs surgery. Surgical treatment is also carried out if conservative therapy did not bring any results.
When do you need a doctor's help?
You should seek medical help for the following symptoms:
- in the presence of deformation, redness, swelling in the shoulder joint or in the place where the subscapular region is located;
- at acute syndrome pain, which is accompanied by impaired breathing, palpitations, lack of air;
- in case of bleeding or fracture of bone tissue;
- for pain that causes dizziness or fainting;
- with impaired breathing.

If at least one of the listed symptoms occurs in a patient with pain and inflammation in the subscapularis muscle, it is important not to hesitate, but to go to the hospital immediately.
Features of therapy
Treatment is prescribed by the doctor, taking into account the causes of pain and inflammation in the subscapular region. If excluded traumatic cause, treatment is carried out with medications or other methods of therapy.
The subscapular region should be treated in the following ways:
- With the help of rest. In some situations, it is enough just to have a good rest so that the muscles can recover and the overstrain in them disappears.
- Inflammatory processes must be eliminated with non-steroidal anti-inflammatory drugs: for example, Movalis, Voltaren or Celebrex.
- If the subscapular region is affected by muscle spasm, muscle relaxants are used.
- Chronic manifestations of pain accompanied by depression are treated with antidepressants.
- Physiotherapy is also used to reduce inflammation in tissues and muscles, relieve pain and improve regeneration.
- Manual treatment is used to remove blocks in muscles and improve mobility of motor segments.
Experienced specialists influence biologically active points, as a result of which pain decreases and normal conduction along nerve fibers is restored.
To remove muscle spasms In the subscapular region, it is recommended to undergo a whole course of massage. Massage actions also help improve blood circulation and overall well-being.
Preventing problems in the subscapularis muscle
Prevention of pain in the area under the shoulder blades is to follow the following recommendations:
- Sleep on a hard bed with a small pillow.
- Every day, perform a set of exercises for all muscles, including the area under the shoulder blades.
- Even if you have slight pain in your back or shoulder, limit the movement of your arm on the side of the pain and be sure to rest.
- During monotonous, rhythmic work, regularly massage the shoulder area, as well as the entire back. For procedures you can use essential oils, warming and relaxing gels.
Daily muscle exercises should not be too long. In the morning it is enough to exercise for 20 minutes. During the day, it is recommended to do three approaches lasting 15 minutes.
Now you know what the subscapularis muscle is, why pain may occur under the shoulder blades, and what treatment can help get rid of it. unpleasant symptoms. You cannot self-medicate. Therapy for pathologies in the subscapular region is prescribed only by a doctor and must be strictly followed.
The scapula is located from the II to VII ribs along the posterior surface of the chest, it is a flat triangular bone with three edges: upper, medial and lateral, which converge and form three angles: upper, lateral and lower. The lateral angle is thickened and forms the neck of the scapula, which passes into the glenoid cavity. Near the cavity, the coracoid process extends from the upper edge. The anterior surface of the scapula is filled with the subscapularis muscle. The posterior surface of the scapula is divided by the spine into two unequally sized fossae: the smaller supraspinatus, filled with the muscle of the same name, and the large infraspinatus, filled with the infraspinatus, teres minor and major muscles. The spine of the scapula, continuing to the lateral side, ends with an acre ion hanging behind and above the glenoid cavity. The deltoid muscle begins from the spine and acromion, and from the coracoid process to the shoulder go the coracobrachialis muscle, the short head of the biceps brachii muscle and the pectoralis minor muscle. The long head of the biceps brachii and the long head of the triceps brachii muscles are attached to the tubercles of the glenoid cavity above and below the cartilaginous zone, respectively.
Starting from the transverse processes of G-Civ with four teeth, the muscle that lifts the scapula goes obliquely down and is attached to the upper corner of the scapula. Two more muscles are attached to the medial edge of the scapula: the rhomboid, which begins from the spinous processes of Cvi-Cvii and Di-Div, and the serratus anterior, which begins with nine teeth from the upper ribs (from I to VIII or IX). This abundance of muscles makes the scapula very mobile. In addition, all of these muscles are involved in abduction, adduction, external and internal rotation of the shoulder, and the trapezius and serratus anterior muscles abduct the shoulder beyond 90°.
Scapula fractures. These fractures account for 0.3-1.5% of all skeletal bone injuries. The fracture line can pass through various anatomical structures of the scapula. In this regard, fractures of the body, spine and angles of the scapula are distinguished. They occur in most cases due to a direct mechanism of injury: a blow to the shoulder blade or a fall on it. With an indirect mechanism (a fall on the hand or elbow joint of the abducted arm), another group of injuries most often occurs: fractures of the glenoid cavity, neck of the scapula, acromion and coracoid process.
Character clinical manifestations depends on the location of the damage. Thus, fractures of the body, spine and angles of the scapula are accompanied by pain, swelling due to hemorrhage - a symptom of a “triangular pillow”; palpation can sometimes reveal deformation, pathological mobility, and crepitus. Limb function is moderately affected.
A fracture of the glenoid cavity is manifested by pain, hemarthrosis, and a sharp dysfunction of the shoulder joint. When the neck of the scapula is fractured with displacement of the fragments, the shoulder joint seems to slide anteriorly and downward. Its contours change. The acromion stands out too much under the skin, and the coracoid process seems to go backwards. Some depression forms under the acromion. Movement in the shoulder joint is possible, but severely limited due to pain. Palpation reveals pain and sometimes crepitus in the area of the neck of the scapula, especially if passive movements are attempted at the same time. The site of injury is accessible to examination from the anterior and posterior surfaces of the axilla. Fractures of the acromion and coracoid process are characterized by swelling at the site of injury, the presence of a bruise (better visible on the 2-3rd day), local pain, and bone crunching, which appear on palpation of the processes. Movements in the shoulder joint are limited, since attempting to perform them causes pain at the fracture sites.
The shoulder blade is covered with muscles, and its outer corner is covered with the tissues of the shoulder joint and is located deep in them. Severe tissue swelling due to edema and hemorrhage, repeating the shape of the scapula (the “triangular cushion” symptom), in some cases complicates research and diagnosis. To avoid possible mistakes, at the slightest suspicion of a fracture of the scapula, it is necessary to take x-rays in two projections - frontal and lateral.
For scapula fractures, a conservative method is used predominantly. Pain relief for all types of fractures is carried out by injecting 10-40 ml of a 1% novocaine solution into the injury site. Fragments of the body, spine and angles of the scapula are displaced slightly and do not require reposition. Apply a Deso bandage with a roller in the armpit for 3-4 weeks. Working capacity is restored after 4-5 weeks. In case of fractures of the neck of the scapula without displacement, fractures of the acromion and coracoid process with displacement, the limb is fixed with an abduction splint or a plaster thoracobrachial bandage. The shoulder is abducted by 80-90° and deviated posteriorly from the axis of the shoulder girdle by 10-15° (Fig. 4.5). The period of immobilization is 4-6 weeks, ability to work is restored after 6-8 weeks.
If the fracture of the scapula neck is displaced, reduction is carried out using skeletal traction on an abduction splint. The pin is passed through the olecranon process. The position of the limb is the same as for non-displaced fractures. Traction lasts 3-4 weeks, then a plaster thoracobrachial bandage is applied for another 3 weeks. The position of fragments during traction is controlled by clinical and radiological methods.
During the period of immobilization, functional and physiotherapeutic treatment is carried out, after which a course of rehabilitation therapy is prescribed. Working capacity for displaced fractures of the scapula neck is restored after 8-10 weeks.
TO surgical treatment Fractures of the neck of the scapula are extremely rare. Indications for open reduction are fractures with unresolved significant displacement of fragments, especially angular ones, when severe dysfunction of the shoulder joint is predicted.
The operation is performed under general anesthesia. The patient is placed on his stomach with his arm abducted. An incision is made parallel to the outer edge of the scapula from the posterior edge of the deltoid muscle to the middle of the medial edge of the scapula. The infraspinatus and teres minor muscles are exposed and bluntly divided. The infraspinatus muscle along with the fascia is divided at the deltoid muscle. By spreading the edges of the wound up and down with hooks, the neck of the scapula is exposed. The fragments are compared and fastened with metal plates. The dissected tissues are sutured in layers. A plaster thoracobrachial cast is applied with abduction and posterior deviation of the shoulder for a period of 6 weeks. Subsequent treatment is the same as with conservative methods.


