Antipyretics for children are prescribed by a pediatrician. But there are emergency situations for fever when the child needs to be given medicine immediately. Then the parents take responsibility and use antipyretic drugs. What is allowed to give to infants? How can you bring down the temperature in older children? What medicines are the safest?
Superficial veins of the lower limb, vv. superficiales membri inferioris, anastomose with deep veins of the lower limb, vv. profundae membri inferioris, the largest of which contain valves.
In the foot area, the saphenous veins form a dense network, which is divided into the plantar venous network, rete venosum plantare, and dorsal venous network of the foot, rete venosum dorsale pedis.
On the plantar surface of the foot, the rete venosum plantare receives efferent veins from the network of superficial plantar digital veins, vv. digitales plantares and intercapitate veins vv. intercapitulares, as well as other veins of the sole, forming arcs of various sizes.

The subcutaneous venous plantar arches and superficial veins of the sole along the periphery of the foot widely anastomose with the veins that run along the lateral and medial edges of the foot and are part of the cutaneous dorsal venous network of the foot, and also pass in the heel area into the veins of the foot and further into the veins of the leg.
In the region of the edges of the foot, the superficial venous networks pass into the lateral marginal vein, v. marginalis lateralis, which passes into the small saphenous vein of the leg, and the medial marginal vein, v. marginalis medialis giving rise to the great saphenous vein of the leg. The superficial veins of the sole anastomose with the deep veins.
On the back of the foot in the region of each toe is a well-developed venous plexus of the nail bed. The veins that drain blood from these plexuses run along the edges of the dorsal surface of the fingers - these are the dorsal digital veins of the foot, vv. digitales dorsales pedis. They anastomose between themselves and the veins of the plantar surface of the fingers, forming at the level of the distal ends metatarsal bones dorsal venous arch of the foot, arcus venosus dorsalis pedis.
This arch is part of the dorsal venous network of the foot. For the rest of the rear of the foot, the dorsal metatarsal veins of the foot stand out from this network, vv. metatarsales dorsales pedis, among them relatively large veins that run along the lateral and medial edges of the foot. These veins collect blood from the dorsal, as well as from the plantar venous networks of the foot and, heading proximally, directly continue into two large saphenous veins of the lower limb: the medial vein into the great saphenous vein of the leg, and the lateral vein into the small saphenous vein of the leg.
1. Great saphenous vein of the leg, v. saphena magna , is formed from the dorsal venous network of the foot, forming as an independent vessel along the medial edge of the latter. It is a direct continuation of the medial marginal vein.

Heading upward, it passes along the anterior edge of the medial malleolus to the lower leg and follows in the subcutaneous tissue along the medial edge of the tibia. Along the way, it takes a number of superficial veins of the lower leg.
Reaching knee joint, the vein goes around the medial condyle from behind and passes to the anteromedial surface of the thigh. Following proximally, it pierces the superficial leaf of the wide fascia of the thigh in the area of the subcutaneous fissure and flows into v. femoralis.
The great saphenous vein has several valves.

On the hip v. saphena magna receives numerous veins that collect blood on the anterior surface of the thigh, and an additional saphenous vein of the leg, v. saphena accessoria, which is formed from the skin veins of the medial surface of the thigh.
2. Small saphenous vein of the leg, v. saphena parva , emerges from the lateral part of the subcutaneous dorsal venous network of the foot, forming along its lateral edge, and is a continuation of the lateral marginal vein.

Then it goes around the lateral ankle from behind and, heading upward, passes to the back surface of the lower leg, where it goes first along the lateral edge of the calcaneal tendon, and then along the middle of the back surface of the lower leg.
On its way, the small saphenous vein, taking numerous saphenous veins of the lateral and posterior surfaces of the leg, anastomoses widely with deep veins. In the middle of the back surface of the lower leg (above the calf) passes between the sheets of the fascia of the lower leg, goes next to the medial cutaneous nerve of the calf, n. cutaneus surae medialis, between heads calf muscle. Having reached the popliteal fossa, the vein goes under the fascia, enters the depth of the fossa and flows into the popliteal vein.
The small saphenous vein has several valves.
V. saphena magna and v. saphena parva widely anastomose with each other.
Region boundaries
upper the border of the anterior region of the thigh is the line connecting the spina iliaca anterior superior and the pubic tubercle (projection of the inguinal ligament);
lower the border of the anterior region of the thigh is a transverse line drawn 6 cm above the patella.
lateral border of the anterior region of the thigh - a line drawn from this spine to the lateral epicondyle of the thigh;
medial border of the anterior region of the thigh - a line running from the pubic symphysis to the medial epicondyle of the thigh
The thigh is divided into anterior and posterior regions according to the lateral and medial borders.
Layers of the anterior thigh
Skin - thin, mobile, taken in folds, rich in sebaceous and sweat glands. On the lateral surface it is thickened and less mobile. Langer's lines on the anteromedial surface go obliquely - from bottom to top and from outside to inside, on the anterolateral surface - in the form of an oval, corresponding to the position of m. tensor fasciae latae. Blood supply due to arteries pkzhk.
Cutaneous nerves: Under the medial part of the inguinal ligament, the femoral branch of the femoral-genital nerve, r. femoralis n. genitofemoralis. Below the superior anterior iliac spine in the subcutaneous tissue passes the lateral cutaneous nerve of the thigh, n. cutaneus femoris lateralis. Cutaneous branch of the obturator nerve, r. cutaneus n. obturatorii, comes along the inner surface of the thigh to the level of the patella.
Subcutaneous tissue well defined on the thigh and superficial fascia, consisting of two sheets, is divided into several layers. In the subcutaneous tissue, in addition to the named cutaneous nerves, there are two groups of superficial lymph nodes(inguinal and subinguinal) and superficial branches femoral artery with accompanying veins: superficial epigastric artery (a. epigastrica superficialis), superficial artery, circumflex ilium (a. circumflexa ilium superficilis), and external pudendal arteries aa. pudendae externae). In addition, on the anteromedial surface of the thigh vertically passes v. saphena magna
Own fascia of the thigh (fascia lata) It is a rather thick fibrous plate, especially on the outside, where the tendon fibers of the tensor fascia lata muscle are woven into it. This thickened section of its own fascia is called the iliotibial tract and is used in surgery to plastic surgery. Surrounding the thigh from all sides, the fascia sends three intermuscular septa to the femur: medial, which, in addition, forms the fascial sheath of the femoral neurovascular bundle, lateral and posterior.
Thus, three fascial receptacles of the thigh are formed. In addition, some muscles have their own fascial sheaths. Between the fascial muscle cases there are interfascial cellular fissures, and between the broad muscles and the femur, there are musculoskeletal fissures. They are connected with each other and with cellular spaces of other areas. Purulent streaks spread almost freely through the following layers of fiber:
- paravasal fiber
- paraneural tissue
- paraossular fiber
muscles
Anterior group - flexors: quadriceps femoris and sartorius
Medial group make up the muscles that bring the thigh: comb muscle, long, short and large adductor muscles, thin muscle.
To the back group hip extensors include: biceps femoris, semitendinosus, and semimembranosus muscles
femur
MUSCLE AND VASCULAR GAPS
muscle gap formed by the iliac crest (outside), the inguinal ligament (in front), the body of the ilium above the articular cavity (behind) and the iliac crest (inside). The iliopectineal arch (arcus iliopectineus - PNA; formerly called lig. Iliopectineum, or fascia iliopectinea) originates from the pupart ligament and attaches to the eminentia iliopectinea. It runs obliquely from front to back and from outside to inside and is closely intertwined with the fascial sheath of the iliopsoas muscle. The shape of the muscle gap is oval. The inner third of the lacuna is covered by the outer edge of the vascular lacuna.
The content of the lacuna is the iliopsoas muscle, which passes in the fascial sheath, the femoral nerve and the lateral cutaneous nerve of the thigh. The long diameter of the lacuna is on average 8–9 cm, and the short diameter is 3.5–4.5 cm.
Vascular lacuna formed in front by the pupart ligament, behind - by the Cooper ligament located along the crest of the pubic bone (lig. Pubicum Cooped; now referred to by the term lig. Pectineale), outside - by the iliac crest, inside - by the jimbernate ligament. The lacuna is triangular in shape, with its apex directed posteriorly to the pubic bone, and its base anteriorly, to the pupart ligament. The lacuna contains the femoral vein (medial position) and the femoral artery (laterally), ramus femoralis n. Genitofemoralis, fiber and Rosenmuller-Pirogov's lymph node. The base of the vascular lacuna is 7–8 cm long and 3–3.5 cm high.
femoral canal (canalis femoralis) is located under the medial part of the pupart ligament, medially from the femoral vein. This term refers to the path that the femoral hernia passes (in the absence of a hernia, the channel as such does not exist). The channel has the shape of a trihedral prism. The internal opening of the canal is formed in front by the pupart ligament, from the inside by the lacunar ligament, from the outside by the sheath of the femoral vein, and from behind by the Cooper (comb) ligament. This opening is closed by the transverse fascia of the abdomen, which in this area is attached to the ligaments that limit the opening, and to the sheath of the femoral vein. A lymph node is usually located at the inner edge of the vein. The outer opening of the canal is an oval fossa. It is covered with a cribriform plate, lymph nodes, the mouth of the great saphenous vein with veins flowing into it.
The channel walls are: outside - a case of the femoral vein, in front - a superficial sheet of the wide fascia of the thigh with the upper horn of its crescent-shaped edge, behind - a deep sheet of the wide fascia. The inner wall is formed by the fusion of both sheets of the fascia lata of the thigh with the fascial sheath of the pectineal muscle. The length of the channel is very small (0.5 - 1 cm). In cases where the superior horn of the falciform fascia merges with the pupartite ligament, the anterior wall of the canal is absent. The external opening of the canal - hiatus saphenus - is a subcutaneous gap in the surface sheet of the wide fascia of the thigh, closed by a cribriform plate (lamina cribrosa). The edges of the hiatus saphenus are formed by compacted areas of the fascia lata: the lower horn, the superior horn, and outside the crescent-shaped edge of the fascia lata. Length of hiatus saphenus 3 - 4 cm, width 2 - 2.5 cm.




FEMORAL TRIANGLE (trigonum femorale) 
The femoral triangle, scarpovsky, or Scarpa's triangle, is limited on the lateral side by the sartorius muscle, m. sartorius, with medial - long adductor muscle, m. adductor longus; its apex is formed by the intersection of these muscles, and its base by the inguinal ligament. The height of the femoral triangle is 15-20 cm. 
Vascular formations of the femoral triangle
Femoral vessels, a. et v. femoralis, enter the femoral triangle from the vascular lacuna medially from the middle of the inguinal ligament. Further, they are located along the bisector of the femoral triangle to its apex. The femoral vessels are surrounded by a dense fascial sheath, passing to their branches.
Topography of the femoral artery
femoralis is a direct continuation of the external iliac artery. Its diameter is 8-12 mm. At the level of the hiatus saphenus, the artery is covered in front by the crescent-shaped edge of the subcutaneous fissure and lies outward from the vein of the same name. Here, three superficial branches depart from the artery: a. epigastric superficialis, a. circumflexa ilium superficialis and aa. pudendae externae superficialis et profundus.
Projection line of the femoral artery
1. The upper point is medial from the middle of the inguinal ligament, the lower one is behind the internal condyle (proposed by Dyakonov)
2. The upper point is one finger diameter medial from the middle of the line connecting the superior anterior iliac spine with the pubic tubercle, the lower one is the internal condyle of the thigh (proposed by Pirogov)
3. The upper point is the border between 2/5 internal and 3/5 external parts of the inguinal ligament, the lower one is the middle of the popliteal fossa (proposed by Bobrov)
4. The upper point is the middle between the spina iliaca anterior superior and the pubic symphysis, the lower one is the tuberculum adductorium of the medial femoral epicondyle (Kane's line)
The pulsation of the femoral artery is determined immediately below the inguinal ligament in the fossa iliopectinea.
Topography of the femoral vein
V. femoralis lies medially from the artery, under the ethmoid fascia, where v. saphena magna and the veins of the superficial arteries of the same name. Further down, the vein gradually moves to the posterior surface of the artery. At the apex of the femoral triangle, the vein is hidden behind the artery.
Projection line of the great saphenous vein
The lower point is the posterior edge of the medial femoral condyle.
The upper point is on the border of the medial and middle thirds of the inguinal ligament.
Deep artery of the thigh, a. profunda femoris, - the main vascular collateral of the thigh - is sometimes equal in diameter to the femoral one. It usually departs from the posterior, less often from the posterior or posterior-internal semicircle of the femoral artery at a distance of 1-6 cm from the inguinal ligament. The vein of the same name is always located medially from the deep artery of the thigh.
femoral nerve at a distance of 3 - 4 cm down from the level of the inguinal ligament is divided into a large number of muscle and skin branches. The largest cutaneous branch is n. saphenus, which accompanies the femoral artery over a greater extent. In the middle third of the femoral triangle n. Saphenus is located laterally from the femoral artery, and in the lower part of the femoral triangle passes anterior to it.
The bottom of the femoral triangle is the iliopsoas and pectus muscles covered with a deep sheet of the broad fascia. The edges of these muscles adjacent to each other form sulcus iliopectineus, which, towards the top of the triangle, passes into sulcus femoris anterior. In this groove are the femoral vessels and n.saphenus. This neurovascular bundle is then directed to the adductor canal.
adductor channel (canalisadductorius) is located under the wide fascia and is covered in front by m. sartorius. posteromedial wall adductor channel is m. adductor magnus, lateral wall of the adductor canal- m. vastus medialis. anteromedial wall of the adductor canal forms a wide adductor intermuscular septum, septum intermusculare vastoadductoria, stretched from the large adductor muscle to m. vastus medialis
In the afferent canal, there are three holes. Through top hole from sulcus femoralis anterior, femoral vessels and n. saphenus. bottom hole represents a gap between the bundles of the large adductor muscle or between its tendon and the femur; through it, the femoral vessels pass into the popliteal fossa. front opening in septum intermusculare vastoadductoria is the exit point from the canal (into the tissue under m. sartorius) of the descending knee artery and vein, a. et v. descendens genus and n. saphenus. Vessels and n. saphenus can exit the canal separately; in these cases, there will be multiple front openings. The length of the adductor canal (canalis adductorius) is 5-6 cm, its middle is 15-20 cm from the tuberculum adductorium femoris on the medial epicondyle of the thigh. In the proximal direction, the adductor canal communicates with the space of the femoral triangle, distally - with the popliteal fossa, along the a et v. descendens genus and n. saphenus - with subcutaneous tissue on the medial surface of the knee joint and lower leg. According to these connections, the spread of purulent processes in this area can occur. The fascial sheath of the femoral vessels is firmly fused with the upper edge of the septum intermusculare vastoadductoria, and below the vessels deviate from this plate by 1.0-1.5 cm, with the femoral artery lying anteriorly and medially, and the vein lying posteriorly and laterally. A. descendens genus (single or double) reaches the arterial network of the knee joint, sometimes forming a direct anastomosis with the anterior recurrent branch of the tibial artery, a. recurrens tibialis anterior. N. saphenus in the subcutaneous tissue of the leg joins v. saphena magna and reaches the middle of the inner edge of the foot.
obturator canal is a groove on the lower surface of the pubic bone, bounded from below by the obturator membrane and muscles attached along its edges. outer hole obturator canal is projected 1.2-1.5 cm down from the inguinal ligament and 2.0-2.5 cm outward from the pubic tubercle. Deep (pelvic) opening of the obturator canal faces the prevesical cellular space of the small pelvis. outer hole obturator canal is located at the upper edge of the external obturator muscle. It is covered by the comb muscle, which has to be dissected when accessing the obturator canal. The length of the obturator canal is 2-3 cm; the vessels of the same name and the nerve pass through it. The obturator artery anastomoses with the medial circumflex femoral artery and with the inferior gluteal artery. The anterior and posterior branches of the obturator nerve innervate the adductor and gracilis muscles, as well as the skin of the medial surface of the thigh.
The back of the thigh, regio femoris posterior
The cellular space of the posterior fascial bed of the thigh communicates proximally with the space under the gluteus maximus muscle - along the sciatic nerve; distally - with the popliteal fossa along the same nerve; with the anterior bed of the thigh - along the perforating arteries and a. circumflexa femoris medialis.
Projection of the sciatic nerve determined by a line drawn from the middle of the distance between the ischial tuberosity and the greater trochanter to the middle of the popliteal fossa.
Harness rules
Clamping of the femoral artery is performed below the middle of the pupart ligament to the horizontal branch of the pubic bone
The tourniquet is used only for damage to the arteries of the extremities.
Do not apply a tourniquet to a bare wound. The lining should not have any wrinkles.
The injured limb is elevated and the artery is pressed with fingers above the wound.
The tourniquet is applied above the wound and as close to it as possible.
The first round should be tight, the subsequent rounds should be fixing.
The tourniquet is applied in a tiled manner, without infringing the skin.
The tourniquet should not be crushing. The approximate force of applying the tourniquet is until the disappearance of the pulse in the artery below the tourniquet.
With a properly applied tourniquet, bleeding should stop, and the pulse on the artery below the tourniquet should not be determined, the skin becomes pale.
Under the last tour of the tourniquet, a note is attached indicating the date and time of its application.
The part of the body where the tourniquet is applied must be accessible for inspection.
Be sure to carry out transport immobilization of the injured limb and anesthesia.
In cold weather, the limb must be insulated to prevent frostbite.
The duration of the application of the tourniquet in the summer is no more than 1.5 hours, in the winter - no more than 1 hour.
If the time has expired, but the tourniquet cannot be removed:
press the damaged artery above the tourniquet with your fingers;
carefully loosen the tourniquet for 20-30 minutes to restore blood circulation in the injured limb;
re-apply a tourniquet, but above or below the previous location and indicate a new time;
if necessary, the procedure is repeated after half an hour or an hour.
Advantages:
Fairly fast and effective method stop bleeding from the arteries of the limb.
Flaws:
The use of a tourniquet leads to complete bleeding distal departments extremities due to compression of not only damaged great vessels, but also collaterals, which for more than 2 hours can lead to gangrene;
The nerve trunks are compressed, which is the cause of post-traumatic plexitis with subsequent pain and orthopedic syndrome;
The cessation of blood circulation in the limb reduces the resistance of infection tissues and reduces their regenerative abilities;
The use of a tourniquet can cause severe angiospasm and lead to thrombosis of the operated artery;
Restoration of blood circulation after the application of the tourniquet contributes to the development of tourniquet shock and acute renal failure.

Typical places for applying Esmarch's tourniquet to stop bleeding.
1 - on the lower leg; 2 - on the thigh; 3 - shoulder; 4 - shoulder (high) with fixation to the body;
5 - on the thigh (high) with fixation to the body
Primary surgical treatment of a soft tissue wound of the thigh
Modern primary surgical treatment of a wound consists of the following elements:
1) disinfection of the surgical field within a radius of up to 10 cm around the wound;
2) anesthesia (general or local - depending on the wound and the condition of the victim),
3) cutting the wound along its long axis to the bottom;
4) revision of the wound cavity by examining it (the wound is opened toothy hooks) 5) removal of foreign bodies from the wound (fragments of metal, wood, clothes, stones, earth, etc.);
6) cutting another scalpel damaged edges of the wound and the bottom within healthy tissues, departing from the edges of 0.5-1.5 cm (the size depends on the location of the wound, i.e. the nature of the tissues - are there any vital vessels, nerves, organs, etc. in the wound area); d.);
7) if it is impossible to completely remove the bottom of the wound (as well as its edges), only the most affected tissues are removed within the anatomical limits;
8) carrying out after the change of gloves and instruments by the surgeon hemostasis in the wound by tying the vessels with threads (mainly those that dissolve) or their electrocoagulation;
9) washing the wound with chemical antiseptics(solutions of furacilin, chlorhexidine, iodopyrone, etc.);
10) introduction of drainage into the wound - a rubber strip or a vinyl chloride or silicone tube (depending on the nature of the wound and the degree of its contamination with microflora);
11) closing the wound with sutures after careful removal of damaged tissues.
Conditions for applying the primary seam after PHO:
Satisfactory condition of the victim
Early and radical primary surgical treatment of the wound.
Absence of signs of an incipient infectious complication of the wound.
Early prophylactic use of antibiotics (the term is ambiguous, debatable).
The possibility of daily monitoring of the victim until the removal of sutures by a qualified surgeon.
The presence of full-fledged skin and the absence of skin tension.
PST uses a common set of tools
Korntsang, is applied to processing of the operational field. There may be two. 2. Linen claws - for holding the dressing. 3. Scalpel - must be both pointed and belly, several pieces, because during the operation they have to be changed, and after the dirty stage of the operation - thrown away. 4. Clips hemostatic Billroth, Kocher, "mosquito", - are used in large quantities. 5. Scissors - straight and curved along the edge and plane - several pieces. 6. Tweezers - surgical, anatomical, pawled, they should be small and large. 7. Hooks (retractors) Farabeuf and serrated blunt - several pairs. 8. Probes - bellied, grooved, Kocher. 9. Needle holder. 10. Different needles - set .
The first attempt to create a classification of the superficial venous network of the lower extremities in our country belongs to the famous domestic anatomist V. N. Shevkunenko (1949). He believed that the reduction of the primary venous network that occurs in embryogenesis leads to the emergence of the main subcutaneous trunks. In accordance with this, he divided all possible variants of the structure into three types: a) the type of incomplete reduction; b) extreme reduction type and c) intermediate type (Fig. 1.3)
Rice. 1.3. Types of variability of the superficial veins of the lower extremities [Shevkunenko VN, 1949]. a - type of incomplete reduction; b - type of extreme degree of reduction; c - intermediate type
If in the superficial venous system, mainly on the lower leg, the intermediate type of structure of the veins dominates, then for the deep veins the main form is the most common, which is the result of an extreme degree of reduction of the primary venous network. With this form, deep veins are represented by two equivalent trunks with a small number of anastomoses between them. With a loose form, the leg veins are multi-stemmed, with a large number of anastomoses. The intermediate form occupies a middle position. All three types of surface structure venous system lower extremities (main, loose and intermediate) have been studied in sufficient detail and do not cause significant controversy. Much more disagreement exists in the description of the structural features of deep veins at various levels of the lower limb, especially their relationship with each other. The origins of the inferior vena cava are the veins of the foot, where they form two networks - the cutaneous venous plantar network and the cutaneous venous network of the rear of the foot. The common dorsal digital veins, which are part of the cutaneous venous network of the rear of the foot, anastomose with each other to form the cutaneous dorsal venous arch of the foot. The ends of this arc continue in the proximal direction in the form of two longitudinal venous trunks: the lateral marginal vein (v. marginalis lateralis) and the medial vein (v. marginalis medialis). The continuation of these veins on the lower leg are, respectively, the small and large saphenous veins.
On the plantar surface of the foot, a subcutaneous venous plantar arch is isolated, which anastomoses widely with the marginal veins and sends intercapitate veins into each interdigital space, which anastomose with the veins that form the dorsal arch. The deep venous system of the foot is formed from paired companion veins that accompany the arteries. These veins form two deep arches: dorsal and plantar. The superficial and deep arches are connected by numerous anastomoses. Anterior tibial veins (vv. tidiales anteriores) are formed from the dorsal deep arch, from the plantar (vv. tidiales posteriores) - posterior tibial veins that receive peroneal (vv. peroneae). Thus, the dorsal veins of the foot pass into the anterior tibial veins, and the plantar medial and lateral form the posterior tibial veins.
Venous valves are found only in the largest veins of the foot. Their localization and number are not constant. The superficial venous system of the foot is connected to the deep system by vessels that do not have valves. This fact is of no small importance in clinical practice, since the introduction of various drugs and contrast agents into the superficial veins of the foot in the distal direction ensures their unhindered entry into the deep venous system of the lower limb. Thanks to this anatomical features it is also possible to measure venous pressure in the deep veins of the foot segment by puncturing the superficial vein of the foot. According to a number of authors, there are about 50 such vessels at the level of the foot, of which 15 are located at the level of the sole.
The venous system of the lower leg is represented by three main deep collectors (anterior, posterior tibial and peroneal) and two superficial - large and small - saphenous veins. Since the main load in the implementation of the outflow from the periphery is borne by the posterior tibial veins, into which the peroneal veins drain, it is the nature of their lesion that determines the severity clinical manifestations violations of the venous outflow from the distal limbs.
The great saphenous vein of the lower limb (v. saphena magna), being a continuation of the medial marginal vein (v. marginalis medialis), passes to the lower leg along the anterior edge of the inner ankle, then runs along the medial edge of the tibia and, bending around the medial condyle of the femur, in the area of the knee joint passes to the inner surface of the thigh.
The small saphenous vein (v. saphena parva) is a continuation of the outer marginal vein of the foot (v. marginalis lateralis). Passing behind the outer ankle and heading upward, the small saphenous vein is first located along the outer edge of the Achilles tendon, and then lies on its posterior surface, approaching the midline of the posterior surface of the leg. Usually, starting from this area, the vein is represented by one trunk, less often by two. On the border of the middle and lower thirds of the lower leg, the small saphenous vein penetrates into the thickness of the deep fascia and is located between its sheets. Having reached the popliteal fossa, it pierces a deep sheet of fascia and flows into the popliteal vein. Less commonly, the small saphenous vein, passing above the popliteal fossa, flows into the femoral vein or tributaries of the deep vein of the thigh, and sometimes ends in any tributary of the great saphenous vein. Often, in its terminal section, the vein bifurcates and flows into the deep or saphenous veins in separate trunks. In the upper third of the lower leg, the small saphenous vein forms numerous anastomoses with the system of the great saphenous vein.
The great and small saphenous veins along their course have a large number of deep branches. The deep veins of the lower leg in its upper third form the popliteal vein, the sources of which are the posterior and anterior tibial veins.
Superficial veins communicate with deep ones through perforating veins or perforators (vv. perforantes). Yu. H. Loder (1803) subdivided these veins into direct ones, connecting the main trunks of the saphenous veins with deep ones, and indirect ones, providing a connection between the tributaries of the saphenous veins and the deep venous highways. Since that time, terminological confusion has persisted in the literature regarding the veins connecting the superficial and deep venous systems. R. Linton defined direct perforating veins as veins connecting superficial veins with deep ones, and communicating ones as veins connecting superficial veins with muscular ones. Often in the literature and practice, the terms "perforators" and "communicants" are considered equivalent and are used arbitrarily. In the domestic literature, it is currently generally accepted to consider direct communicating veins flowing into the main trunks of deep veins, and indirect - communicating veins connecting superficial veins with muscle tributaries of deep veins. Perforating refers to the departments of communicating veins at the level of passage (perforation) of the own fascia of the lower leg. Many authors combine the concepts of perforating and communicating veins into a single group of internal perforating veins. Starting from the surface with one or more tributaries, after confluence, the trunk of the vein passes through the fascia, flowing into a deep or muscular vein on its own or dividing into branches. In this regard, some authors distinguish several forms of communicating veins, respectively: simple, complex, atypical, branching and collecting. Other researchers believe that the perforator vein provides a directed transfer of blood from the axes of the superficial veins to the deep veins by perforating the superficial aponeurosis. The communicating vein contributes to the indifferent diffusion of blood between different axes or sections of the superficial veins into the supraaponeurotic spaces. At the same time, these veins are subdivided according to the main topographic groups - medial, lateral and posterior.
Up to 155 perforators, called "permanent" perforators, are described in each lower limb and are detected in at least 75% of studies and surgical interventions for varicose veins. The connection between the subcutaneous and deep veins is carried out mainly indirectly, that is, through the muscular veins. The number of direct communicating veins on the lower leg ranges from 3 to 10. There are much more indirect communicating veins than direct ones. Most of the perforators are located along the axes of the "power" lines. This arrangement meets the functional need. The simplest perforator vein complex is the simple Cockett vein. It contains: 1) a supraaponeurotic segment originating in the nearest axis of the superficial vein; 2) a transaponeurotic segment, perforating the superficial aponeurosis through a larger or smaller lumen, allowing in some cases to provide passage together with the vein of the arteriole and nerve branch; 3) subaponeurotic segment, very quickly ending in the nearest axis of the deep vein; 4) valvular apparatus, classically including one or two supraaponeurotic valves, one or three subaponeurotic valves, an obligatory element of which is the presence of an attachment ring corresponding to the thickening of the venous wall.
The diameter of communicating veins is also variable. According to various data, normally it ranges from 0.1 to 4 mm. At pathological processes ectasia of communicating veins can reach 7-8 mm or more. From the point of view of practical surgery, in our opinion, the classification of the French phlebological school is the most acceptable. They divide perforating veins into minimal (1-1.5 mm), medium (2-2.5 mm) and volumetric (3-3.5 mm). The term "megavena" is used for vessels with a diameter of more than 5 mm.
Thanks to the latest anatomical, ultrasound and endoscopic studies of the venous system of the lower extremities, it became possible to clearly recognize the venous valves, which look like a transparent veil and are able to resist the powerful hemodynamic shocks of the muscle pumps. The number, localization and orientation of the cusps of the valve structures of the veins are also quite variable. The statement that all veins connecting the superficial and deep venous systems have valves that allow blood to pass only into the depth cannot be considered absolutely reliable, since valveless perforating veins were found on the foot and lower leg. There are also valves in the veins of the leg, the valves of which are oriented towards the superficial veins in some cases and in the opposite direction in others. Functioning passively depending on the direction of blood flow, the valvular apparatus of the veins of the lower extremities prevents retrograde discharge of blood, protecting venules and capillaries from a sharp pressure drop during the work of the muscular-venous mechanisms of the foot, lower leg and thigh. Hence the mutual dependence of the localization and function of the valves.
Significant variability in the structure of the superficial venous network of the lower extremities is exacerbated by the discrepancy in the names of veins and the presence of a large number of eponyms, especially in the names of perforating veins. To eliminate such discrepancies and create a unified terminology for the veins of the lower extremities, the International Interdisciplinary Consensus on venous anatomical nomenclature was created in 2001 in Rome. According to him, all the veins of the lower extremities are conventionally divided into three systems:
- superficial veins.
- Deep veins.
- perforating veins.
Superficial veins lie between the skin and the deep (muscular) fascia. At the same time, the GSV is located in its own fascial case, formed by splitting the superficial fascia. The MPV trunk is also located in its own fascial case, the outer wall of which is a superficial sheet of muscular fascia. Superficial veins drain approximately 10% of the blood from the lower extremities. Deep veins are located in spaces deeper than this muscular fascia. In addition, deep veins always accompany the arteries of the same name, which does not happen with superficial veins.

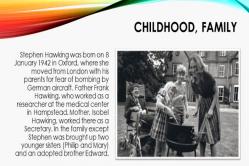
Rice. 1.24. Superficial veins of the lower extremities
Deep veins provide the main blood drainage - 90% of all blood from the lower extremities flows through them. Perforating veins perforate the deep fascia, connecting the superficial and deep veins. The term "communicant veins" is reserved for veins that connect one or another vein of the same system (i.e., either superficial to each other, or deep to each other).
Major superficial veins:
1. Great saphenous vein (GSV) - vena saphena magna, in English literature - great saphenous vein (GSV). Its source is the medial marginal vein of the foot. It goes up the medial surface of the lower leg, and then the thigh. It drains into the BV at the level of the inguinal fold. Has 10-15 valves. The superficial fascia splits into two sheets, forming a channel for the GSV and cutaneous nerves. On the thigh, the GSV trunk and its large tributaries in relation to the fascia can take three main types of mutual arrangement: - i-type, in which the GSV trunk lies entirely subfascially from the SPS to the knee joint; - h-type, in which the trunk of the GSV accompanies a large tributary located suprafascially. In a certain place, it perforates the fascia and flows into the GSV. Distal to this place, the trunk of the GSV is, as a rule, much smaller in diameter than its tributary; - s-type, the extreme degree of the h-type, while the trunk of the GSV distal to the confluence of the tributary is aplastic. At the same time, it seems that the trunk of the GSV at some point abruptly changes direction, perforating the fascia. The existing fascial canal is considered by many authors as a protective outer “cover” that protects the trunk of the GSV from excessive stretching when pressure increases in it.
2. Most permanent tributaries:
2.1 . Intersaphenous vein(s), in the English literature - intersaphenous vein(s) - goes (goes) along the medial surface of the leg. Connects BPV and MPV. It often has connections with the perforating veins of the medial surface of the lower leg.
2.2 . Posterior thigh circumflex vein (vena circumflexa femoris posterior) It can have its origin in the MPV, as well as the lateral venous system. It rises from the back of the thigh, wrapping around it, and drains into the GSV.
2.3 . The anterior vein surrounding the thigh (vena circumflexa femoris anterior), in English literature - anteri or thigh circumflex vein. It may originate in the lateral venous system. It rises along the anterior surface of the thigh, bending around it, and drains into the GSV.
2.4 . Posterior accessory great saphenous vein (vena saphena magna accessoria posterior) This is the name of any venous segment on the thigh and lower leg, running parallel and posterior to the GSV.
2.5. Anterior accessory great saphenous vein (vena saphena magna accessoria anterior), in English literature - anterior accessory great saphenous vein. This is the name of any venous segment on the thigh and lower leg, running parallel and anterior to the GSV.
2.6. Superficial accessory great saphenous vein (vena saphena magna accessoria superficialis), in English literature - superficial accessory great saphenous vein. This is the name of any venous segment on the thigh and lower leg, running parallel to the GSV and more superficial relative to its fascial sheath.
3. Small saphenous vein (vena saphena parva), in English literature - small saphenous vein. It has its source in the external marginal vein of the foot. It rises along the posterior surface of the lower leg and flows into the popliteal vein, most often at the level of the popliteal crease. It receives the following tributaries:
3.1. Superficial accessory small saphenous vein (vena saphena parva accessoria superficialis), in English literature - superficial accessory small saphenous vein. Runs parallel to the MSV trunk above the surface sheet of its fascial sheath. Often flows into the popliteal vein on its own.
3.2. Cranial extension of the small saphenous vein (extensio cranialis venae saphenae parvae), Previously called the femoral-popliteal vein (v. femoropoplitea). It is a vestige of the embryonic intervenous anastomosis. When there is an anastomosis between this vein and the posterior femoral vein from the GSV system, it is called the vein of Giacomini.
4. Lateral venous system (systema venosa lateralis membri inferioris), in English literature - lateral ve nous system. It is located on the anterior and lateral surface of the thigh and lower leg. It is assumed that it is a vestige of the system of the lateral marginal vein that existed in the embryonic period.
5. Inguinal venous plexus (confluens venosus subinguinalis), in English literature - confluence of su perficial inguinal veins. Represents the terminal section of the GSV near the anastomosis with BS. Here, in addition to the last three tributaries listed, three fairly constant tributaries flow: the superficial epigastric vein (v. epigastrica superficialis), the external pudendal vein (v. pu denda externa) and the superficial vein surrounding the ilium (v. circumflexa ilei superficialis). In the English-language literature, there is a long-established term Crosse, which denotes this anatomical segment of the GSV with the listed tributaries.

Rice. 1.5. Perforating veins of the lateral and posterior surfaces of the lower extremities

Rice. 1.6. Perforating veins of the anterior and medial surfaces of the lower extremities
Undoubtedly, only the main clinically significant venous collectors are listed and have their own names. Given the high diversity of the structure of the superficial venous network, other superficial veins not included here should be named according to their anatomical localization. Deep veins, as already mentioned, are located deeper than the muscular fascia and often accompany the arteries of the same name.
Perforating veins are one of the most numerous and diverse venous systems in form and structure. In clinical practice, they are often called by the names of the authors involved in their description. This is not only inconvenient and hard to remember, but sometimes historically not entirely correct. Therefore, in the above international consensus, it is proposed to name perforating veins according to their anatomical location.
Thus, all perforating veins of the lower extremities should be divided into 6 groups, which are divided into subgroups:
1. Perforating veins of the foot
1.1. Dorsal perforating veins of the foot
1.2. Medial perforating veins of the foot
1.3. Lateral perforating veins of the foot
1.4. Plantar perforating veins of the foot
2. Perforating veins of the ankle
2.1. Medial perforating veins of the ankle
2.2. Anterior perforating veins of the ankle
2.3. Lateral perforating veins of the ankle
3. Perforating veins of the leg
3.1. Medial perforating veins of the leg
3.1.1. Paratibial perforating veins
Anatomy and projection of the femoral veins helps to understand the structure of the circulatory system. The vascular network provides an approximate scheme, but differs in variability. Each person has a unique venous pattern. Knowledge of structure and function vascular system, will help to avoid diseases of the legs.
Anatomical structure and topography of veins
The head center of the circulatory system is the heart. Vessels depart from it, which rhythmically contract and pump blood through the body. To the lower extremities, the fluid rapidly enters through the arteries, and returns measuredly back through the veins.
Sometimes these two terms are mistakenly confused. But the veins are responsible only for the outflow of blood. There are 2 times more of them than arteries, and the movement is calmer here. Due to the fact that the walls of such vessels are thinner and the location is more superficial, veins are used to take biomaterial.
The channel of the system is a tube with elastic walls, consisting of reticulin and collagen fibers. Due to the unique properties of the fabric, it retains its shape well.
There are three structural layers of the vessel:
- intima - the inner cover of the cavity, located under the protective shell;
- media - the central segment, consisting of spiral, smooth muscles;
- adventitia - the outer cover in contact with the membrane of muscle tissue.
Elastic partitions are laid between the layers: internal and external, creating the border of the covers.
The walls of the vessels of the femoral limbs are stronger than in other parts of the body. Strength is due to the placement of the cores. The channels are laid in the subcutaneous tissue, therefore they withstand pressure drops, as well as factors affecting the integrity of the tissue.
Functions of the venous network of the thigh
Features of the structure and location of the venous network of the lower extremities endow the system with the following functions:
- The outflow of blood containing waste products of cells and carbon dioxide molecules.
- Supply of synthesized glands, hormonal regulators, organic compounds, nutrients from gastrointestinal tract.
- Circulation of blood circulation by means of a valvular system, thanks to which the movement resists the force of gravity.
With pathologies of the venous vessels, circulatory failures occur. Violations cause stagnation of the biomaterial, swelling or deformation of the pipes.
Projection views of the femoral veins
 An important position in the anatomical projection of the venous system is occupied by valves. The elements are responsible for the correct direction, as well as the distribution of blood along the channels of the vascular network.
An important position in the anatomical projection of the venous system is occupied by valves. The elements are responsible for the correct direction, as well as the distribution of blood along the channels of the vascular network.
The veins of the femoral limbs are classified by type:
- deep;
- superficial;
- perforating.
Where do the deep vessels pass?
The mesh is laid deep from the skin, between muscle and bone tissues. The deep vein system runs through the thigh, lower leg, and foot. Up to 90% of the blood flows through the veins.
The vascular network of the lower extremities includes the following veins:
- sexual lower;
- iliac: external and common;
- femoral and common femoral;
- popliteal and paired branches of the lower leg;
- sural: lateral and medial;
- peroneal and tibial.
The channel begins at the back of the foot from the metatarsal vessels. Further, the fluid enters the tibial anterior vein. Together with the back, it articulates above the middle of the leg, uniting into the popliteal vessel. The blood then enters the popliteal femoral canal. 5–8 perforating branches also converge here, originating from the muscles of the back of the thigh. Among them are lateral, medial vessels. Above the inguinal ligament, the trunk is supported by the epigastric and deep veins. All tributaries flow into the iliac external vessel, which merges with the internal iliac branch. The channel directs blood to the heart.
A separate wide trunk passes the general femoral vein, consisting of a lateral, medial, large subcutaneous vessel. There are 4–5 valves on the core section that set the right movement. Sometimes there is a doubling of the common trunk, which closes in the region of the ischial tuberosity.
The venous system runs parallel to the arteries of the lower leg, foot and fingers. Going around them, the channel creates a duplicated branch.
Scheme and tributaries of superficial vessels
 The system is laid through the subcutaneous tissue under the epidermis. The bed of the superficial veins originates from the plexus of the vessels of the toes. Moving upward, the stream is divided into a lateral and medial branch. The canals give rise to two main veins:
The system is laid through the subcutaneous tissue under the epidermis. The bed of the superficial veins originates from the plexus of the vessels of the toes. Moving upward, the stream is divided into a lateral and medial branch. The canals give rise to two main veins:
- large subcutaneous;
- small subcutaneous.
Great saphenous vein of the thigh- the longest vascular branch. Up to 10 pairs of valves are located on the grid, and the maximum diameter reaches 5 mm. In some people, a large vein consists of several trunks.
The vascular system passes through the lower extremities. From the back of the ankle, the channel stretches to the lower leg. Then, bending around the internal condyle of the bone, it rises to the oval opening of the inguinal ligament. The femoral canal originates in this area. Up to 8 tributaries also flow here. The main ones are: external genital, superficial epigastric and iliac vein.
Small saphenous vein the channel begins on the front side of the foot from the marginal vessel. Bending around the ankle from behind, the branch stretches along the back of the lower leg to the popliteal region. From the middle of the calf, the trunk runs along connective tissues limbs in parallel with the medial cutaneous nerve.
Due to additional fibers, the strength of the vessels increases, therefore, a small vein, unlike a large one, is less likely to undergo varicose expansion.
Most often, the vein crosses the popliteal fossa and flows into the deep or great saphenous vein. But in a quarter of cases, the branch penetrates deep into the connective tissues and articulates with the popliteal vessel.
Both surface trunks receive tributaries in different areas in the form of subcutaneous and skin channels. Between themselves, the venous tubes communicate with the help of perforating branches. At surgical treatment diseases of the legs, the doctor needs to accurately determine the anastomosis of the small and deep veins.
Location of the perforating grid
 The venous system connects the superficial and deep vessels of the thigh, lower leg, and foot. The branches of the mesh pass through soft tissues, penetrating the muscles, therefore they were called perforant or communicant. The trunks have a thin wall, and the diameter does not exceed 2 mm. But with a lack of valves, the partitions tend to thicken and expand several times.
The venous system connects the superficial and deep vessels of the thigh, lower leg, and foot. The branches of the mesh pass through soft tissues, penetrating the muscles, therefore they were called perforant or communicant. The trunks have a thin wall, and the diameter does not exceed 2 mm. But with a lack of valves, the partitions tend to thicken and expand several times.
Perforator mesh is divided into two types of veins:
- straight;
- indirect.
The first type connects the tubular trunks directly, and the second - through additional vessels. The mesh of one limb consists of 40–45 penetrating channels. The system is dominated by indirect branches. Straight lines are concentrated in the lower part of the lower leg, along the edge of the tibia. In 90% of cases, pathologies of perforating veins are diagnosed in this area.
Half of the vessels are equipped with directional valves that send blood from one system to another. Stop veins do not have filters, so the outflow here depends on physiological factors.
Indicators of the diameter of venous vessels
The diameter of the tubular element of the lower extremities ranges from 3 to 11 mm, depending on the type of vessel:
The diameter of the vessel depends on the muscle tissue laid in the area under study. The better developed the fibers, the wider the venous tube.
The indicator is affected by the serviceability of the valves. When the system is disturbed, a jump in blood outflow pressure occurs. Prolonged dysfunction leads to deformation of the venous vessels or the formation of clots. Commonly diagnosed pathologies include varicose veins, thrombophlebitis, and thrombosis.
Diseases of the venous vessels
 According to the WHO, pathologies of the venous system are registered in every tenth adult. The number of young patients is growing every year, and disorders are found in schoolchildren. Diseases of the circulatory system of the lower extremities are most often caused by:
According to the WHO, pathologies of the venous system are registered in every tenth adult. The number of young patients is growing every year, and disorders are found in schoolchildren. Diseases of the circulatory system of the lower extremities are most often caused by:
- overweight;
- hereditary factor;
- sedentary lifestyle;
The most common dysfunctions of the venous system of the lower extremities:
Varicose veins - valvular insufficiency, and as a result, deformation of the small or large saphenous veins. It is more often diagnosed in women over 25 years of age who have a genetic predisposition or are overweight.
The operation is very traumatic.
There are many classifications of this process. According to the location, the hernia of the cervical, thoracic and lumbar regions is divided. The most common vertebral hernias are located at the level of the lower back. By size:
- All readings are divided into absolute and relative.
- The main symptoms are constant pain in the back and lower back, aggravated by any physical activity. As the disease progresses pain begin to spread to the buttocks, thigh, shins, foot, weakness appears. If you notice numbness or tingling in your legs, this may also indicate the formation of a herniated disc in the lumbar region.
- But this technique also has a number of negative points:
- microdiscectomy;
- Central Clinical Hospital No. 1 "Russian Railways": from 15 thousand rubles (laser vaporization / laser reconstruction).
Consultation of a general practitioner, neurosurgeon, anesthetist.
The size of the hernia exceeds 6 mm.
laser treatment considered pathology includes 2 methods. Both methods are recommended by experts for early dates ailment (within 6 months after the formation of a hernia), when the diameter of the hernia does not exceed 6 mm. The use of a laser will be useful if medical treatment of intervertebral hernia was ineffective, the patient has no contraindications to laser treatment.
- Laser treatment
- large (up to 6 mm and up to 12 mm, respectively);
- Hernia sequestration;
- The rehabilitation period can be slowed down due to the formation of various scars and adhesions in the spinal canal.
- Disc hydroplasty.
Central Clinical Hospital of the Russian Academy of Sciences: from 60 thousand rubles. Anesthesia of the operated area (local anesthesia).
The patient leads an inactive (sedentary) lifestyle. Text
- Laser vaporization (removal) of spinal hernia
- Complications that appear during the operation depend on the qualifications of the operating team, the type of surgical intervention, and the quality of the equipment. The most common complications:
The essence of this method is to enter the damaged disk with a light guide, it heats the core of the disk, the liquid evaporates. Consequently, the hernia also decreases in size. This operation is used for uncomplicated disease. What are the main advantages of this treatment method:
- very large.
- Inability to control urination and bowel movements;
- Endoscopic surgery is a treatment intervertebral hernia in a minimally invasive way, which is carried out through punctures, which minimally injures the tissues, muscles and bone structures of the spine. This reduces the risk of cicatricial adhesions and complications that are possible with other types of operations.
- One of the most effective methods treatment of intervertebral hernia at an early stage - disc hydroplasty. The operation is performed using a special needle. A sterile solution is injected into the disc cavity, which helps flush out the dead tissues of the spinal disc and remove them from the body. The operation takes about a third of an hour. Disc hydroplasty is not done when determining a hernia big size or with ruptures of the fibrous ring.
During a radical operation, not only a hernia is removed, but also an intervertebral disc with pathology. This type of operation is performed at the stages of a sequestered hernia or at the stage of a true hernia (disc prolapse). Garant Clinic: from 80 thousand rubles.
- Insertion of a needle of a special diameter into a damaged disc. To bring the needle to the desired area, the skin is pierced.
- To date, there are many different methods for the treatment of the pathology in question.
- shown in the following cases:
During surgery, the hard shell can be damaged spinal cord. If the doctor is qualified, then he notices this and sutures during the operation. Otherwise, the postoperative period is complicated by severe headaches. The reason is a decrease in intracranial pressure due to leakage of CSF from the spinal canal. The headache will stop after the spontaneous overgrowth of this damage.
The structure of the spinal disc does not change.
The patient has unbearable pain that lasts more than six months. And drug treatment does not help to eliminate them.
- Relative readings:
- Every surgical method has negative consequences. The most common complication after surgery is hernia recurrence. In the postoperative period, recovery is especially important for the patient.
- This type of operation should be carried out only in the presence of absolute indications. About 20% of patients leave bad reviews about the results of this surgical method.
- The most famous among them are the following institutions:
Manipulation is controlled using an X-ray machine, the radiation exposure of which is minimal.
Injuries to the spine when using a laser are minimal, but in the future, due to the destruction of the disk structure, the fusion of the vertebrae with each other, the restoration of the previous biomechanics of the spine may not occur.
- Periodic / constant tingling, burning in the back, neck.
- In the postoperative period, if the prescriptions of the attending physician are not followed, the following complications may occur:
Not the effectiveness of conservative treatment.
- Therefore, if during this period the patient begins to perform various physical activities too early or is injured, there is a high probability of relapse.
- Microdiscectomy - neuro surgical intervention, with the help of which the removal of hernias is carried out. The operation is always performed under anesthesia. Before the operation, it is necessary to undergo an MRI examination or computed tomography.

Research Institute of Traumatology and Orthopedics. Harmful.
The technology of laser treatment of spinal hernia (laser percutaneous reconstruction) differs from laser vaporization:
- The procedure is performed without the use of anesthesia. In some cases (pregnancy, lactation, allergies to certain medications), this may be useful, however, during the manipulation, the patient may feel discomfort.
- Violation of sensitivity.
- Not a long stay inpatient treatment(up to 2 days).
Various purulent-septic local (osteomyelitis or epiduritis) and general (pneumonia, sepsis) complications.
It is not possible to accurately direct the laser beam, therefore, nearby tissues are often damaged.
The underlying disease was complicated by serious disorders on the part of internal organs, for example, from the gastrointestinal tract (fecal incontinence) or the urinary system (urinary incontinence).
- If we talk about the period of recovery and complete recovery of the patient, then in order for this to happen as quickly as possible, the doctor may advise resorting to such concomitant methods of recovery as physiotherapy exercises, massages, manual therapy.
- Then, for some time, what is the essence of the whole process is performed - the laser acts on damaged tissues.
- , then it refers to:
- Treatment of spinal hernia is a process that requires time, patience and professionalism of the attending physician. All treatment can be conditionally divided into the following points:
Since the operation to remove the intervertebral hernia is quick (about an hour), the removal takes place under spinal anesthesia, which reduces the time to recover from anesthesia. The recovery period is very short - the patient after endoscopic surgery gets on his feet in a few hours. Full return to active life occurs after 7-10 days.
- The most accurate diagnostic method that allows not only to identify a hernial formation, but also makes it possible to accurately determine the stage of development of the disease, to see the condition of the vertebrae, the direction of the protrusion of the disc. In addition, with the help of magnetic resonance imaging, we can develop the most correct ways to treat herniated discs. This safe and painless method is today considered the "gold standard" for diagnosing spinal diseases.
- During this period, complex treatment, exercise therapy, physiotherapy are prescribed. Spa treatment is also recommended.
- Thromboembolism may occur.
- The high cost of the operation.
The postoperative period is long. During this time, the muscles of the back are weakened. They can not properly support the spine. The result is a relapse of the disease.
Atrophic changes in the muscular apparatus of the limbs or progressive paralysis. As a rule, such measures are developed individually for a particular patient, taking into account physiological features the patient's body, how the disease proceeded, the age and weight of the patient, the severity of the disease.
- Vaporization involves vaporizing the core of the disc (the steam is expelled through a special needle), and reconstruction involves stimulating those areas of the core that are damaged.
- Physiotherapeutic procedures such as ultrasound, paraffin therapy, magnetotherapy, diadynamic currents, electrophoresis and more;
- Removal of pain syndrome and reduction of tissue swelling;
- Intervertebral hernia operation - the cost of surgical intervention in this regard varies from 80 to 130 thousand rubles.
- It is used if the patient is contraindicated for magnetic resonance therapy (for example, if a pacemaker is installed).
- If the pain does not go away within a week and is not stopped by painkillers, you may have a herniated disc, the treatment of which should be carried out only in a clinical setting.
FedyaUser
Vladimir Vorotyntsev
Sharp movements of the spine are unacceptable.
Doctor StupinDoctor
During the operation, the nerve root is inadvertently damaged. The consequence is paresis or paralysis of the limb, which manifests itself already in postoperative period recovery.
PolinaNewbie
If there are any inflammatory processes, then they are not treated with this method.
nuwa Active user
Radical spinal hernia surgery involves the complete removal of not only the hernia, but also the damaged disc. The vertebrae are connected to each other motionlessly. radical operations shown with sequestered (intervertebral disc falls into the canal of the spinal cord) and fully formed true hernias.
PolinaNewbie
very large.
- The effectiveness of the operation is high only in cases where the patient consults a doctor in a timely manner, but if the stage of the disease is advanced, then re-formation of a spinal hernia is possible;
nuwa Active user
Only an experienced neurosurgeon can perform such an operation in an operating room fully equipped with modern equipment, which is necessary for this kind of manipulation. B vitamins, which will restore the nerve conduction of the spine. Muscle spasm, as a result of which some stiffness in movements is felt;
- Our clinic employs highly qualified specialists with unique experience in the field of microsurgical, endoscopic and puncture methods of treatment of intervertebral hernia.
- On the video treatment of the spine with a laser:
FedyaUser
In addition to the advantages of laser hernia treatment, this method also has disadvantages. Since this is not a radical method, the disc reduction is insignificant, so it may be necessary to repeat the same procedure in the future. In addition, laser therapy takes place with the use of local anesthesia, so the patient may feel some discomfort in the treated area while the doctor is working.
Vladimir Vorotyntsev Physician - manual therapist, rehabilitation specialist
Doctor StupinDoctor
Laser hernia removal has an analgesic effect after the first procedure and increases the likelihood of a good treatment result;
PolinaNewbie
During the operation, young chondrocytes slowly begin to replace the damaged tissue. In some cases, laser irradiation is also used in the case of surgical excision of a hernia, because this method leads to improved tissue healing, many consider it a necessary prevention of recurrence.
nuwa Active user
PolinaNewbie
They kneaded my foot every day, doing a light massage;
- First review from me:
nuwa Active user
In the evening before the operation, it is necessary to clean the intestines. You can give yourself into the hands of the medical staff, and they will make a traditional enema. You can buy a mini enema at the pharmacy and carry out the procedure yourself. Then there was an MRI, which was diagnosed as "... herniated disc L4 - L5, 0.7 cm." Then the conclusion of the VKK, which I wrote about at the beginning of the article.“You are strongly recommended to remove the intervertebral hernia, otherwise you will soon be moving in a wheelchair and walking in a diaper,” this was the verdict of the medical advisory commission after viewing my MRI images.
- Many people believe that the treatment of intervertebral hernias ends with a rehabilitation period. But in order to avoid the recurrence of a hernia in the spine, it is necessary to lead a correct lifestyle. First of all, you need:
Basic principle of laser treatment
Removal of a hernia of the spine
time spent in the hospital, a set of rehabilitation measures, the use of high-tech equipment, the type of anesthesia. A hernia in the later stages leads to compression of the spinal canal, so a more complex complex operation has to be performed: decompression of the spinal cord with microsurgical removal of the hernia (174,000 rubles).
The choice of treatment methods depends on the stage of development of the disease. With timely access to a doctor, treatment can be conservative, very effective at an early stage of the disease. The main therapeutic procedures are massage, exercise therapy, hardware traction and other techniques. Read more on this page.
- The patient spends a minimum period of time in the clinic;
- There are different kinds herniated disc surgery:
- Among the Moscow healthcare institutions, the most famous are
Electrocardiogram.
The mobility of the spine is preserved.
Conservative treatment, which lasted about 3 months, practically positive results did not bring.
A hernia of the spinal column is a rather serious disease. The consequence of the displacement of the intervertebral disc may be a decrease in the lumen of the spinal canal, which leads to prolonged compression of the membrane and roots of the spinal cord. The result is an inflammatory process. The first symptom of this disease fast fatiguability. Then comes the pain. Often very strong. By its irradiation, it is possible to determine the place of formation of the vertebral hernia.
- Almost complete absence of postoperative scars and scars.
- If the patient decides to perform laser removal of the intervertebral hernia, then the attending physician must prescribe an examination of the patient's body, which includes the following steps:
- Includes drug and non-drug therapy, which an experienced specialist will advise to use in combination. Well drug treatment must necessarily include the appointment of such drugs:
With this disease, a gap forms in the fibrous ring, from which part of the nucleus pulposus begins to protrude. It is believed that this disease can be the result of neglected osteochondrosis, and if it is not treated in a timely manner, then a person may temporarily lose his ability to work, and in some cases even become disabled.
The effectiveness of treatment, according to the reviews of patients and doctors, may be different. In some cases, laser therapy for a hernia in different parts of the lower back helps, in others it does not. Each case is individual, since the symptoms, as well as the course of the disease for each patient, have their own characteristics.
Laser vaporization of an intervertebral hernia is based on inserting a needle through the skin, i.e. make a puncture in the disk, and pass a laser LED there. Dosed energy is launched through it, which should turn the liquid in the disk into steam, which will exit through the needle, which helps to reduce the internal pressure in the disk.
Symptoms indicating the presence of the disease
An intervertebral hernia in the early stages may not give itself away. The first symptoms that indicate the presence of the disease appear with its progression. So, here are the main symptoms to look out for:
- strong pain syndrome;
- muscle spasm, as a result of which some stiffness in movements is felt;
- sensory disturbance in the lower extremities;
- leg numbness, tingling and burning sensation.
How is a hernia treated with a laser?
How is laser treatment of spinal hernia performed? Before starting therapy for a hernia of the lumbar spine or sacrum, the patient is sent for testing, diagnostic study to confirm the diagnosis. If there are no contraindications for manipulation, then laser surgery will be prescribed.
Laser vaporization of a hernia is performed only under local anesthesia, since getting rid of a lumbar hernia does not require the use of general anesthesia.
After the operation, the patient must stay in the hospital for another day under constant medical supervision. Only in the evening after laser therapy for a hernia of the lower back or sacral spine can you walk, before that the patient must lie down. The doctor after examining the patient will decide whether or not to let the patient go home. If all is well, then 24 hours after the intervention, the person is discharged home.
Postoperative rehabilitation involves the passage of a medical course.
Within 2 weeks, the patient is treated with anti-inflammatory drugs. nonsteroidal drugs(Movalis, Celebrex, Nimesil).
The doctor prescribes the schedule and dosage of admission, it is forbidden to change prescriptions on your own.
For a whole month you can not visit the office of physiotherapy procedures. Forbidden:
- massage;
- electroprocedures;
- balneotherapy.

Sometimes magnetotherapy and laser therapy are prescribed to enhance the effect of the operation.
You can not visit the pool or gym, physical activity is excluded, which can cause injury to any part of the spine. Working in the country or moving furniture is strictly prohibited.
It is worth walking a lot, doing household chores, walking. Long driving is prohibited. You can spend no more than 40 minutes driving a day. You need to wear a semi-rigid corset for a whole month to reduce the load on the operated spine.
It is possible to fully evaluate the effectiveness of hernia vaporization using laser therapy only after 2 months, although some relief occurs immediately. It is impossible to violate the doctor's recommendations so that the scarring of the fibrous ring proceeds normally, the pressure inside the discs normalizes. After 2 months the patient passes comprehensive examination to adjust the treatment.
If laser therapy does not help, then the hernia can be treated in other ways. Most often, surgery is prescribed to completely remove the hernia. After such operations, a person must change his lifestyle, adjust his diet, take care of his spine, and take preventive measures to prevent the recurrence of a hernia.
Discectomy and laminectomy are the main methods of radical surgical therapy
Under the laser method of treatment is meant the impact on a certain area by a directed beam of photons (light). The power of such a procedure is controlled by the photon wavelength settings.

A low-power laser simply enhances the regenerative capabilities of the body in a particular focus, simultaneously increasing blood circulation. A more powerful laser works differently. It simply destroys the tissues it is directed at (both soft and bone).
Chronic pain is the main indication for hernia vaporization
To remove a herniated disc of the spine, special laser devices are used. The light flux generated by them ignores soft tissues, passing through them and affecting only bone structures (the skin itself remains unharmed).
Can any hernia of the spine be treated with a laser? In most cases, the procedure is not required at all, the disease is treated conservatively. But for removal with a laser, weighty indications are required.
Indications for laser hernia removal:
- Frequently exacerbated pain syndrome.
- Constant feeling discomfort in the back (burning, twitching and tingling, stiffness in movements).
- Violations of the sensitivity of the limbs or back, the development of paresthesia (numbness).
- The occurrence of periodic or even more permanent dizziness, headaches (with damage to the cervical region).
- Threat of bone tissue infection (usually against the background of lumbar or chest lesions).
to the menu
Contraindications
Laser treatment has a number of relative and absolute contraindications. Ignoring them can lead to severe consequences, up to disability.
Herniated disc
List of contraindications:
- the patient's age is more than 50 years;
- the presence of ossification of the pulpous nucleus;
- the presence of a neurological deficit, clinical signs spinal cord injury;
- specific violation of the integrity of the fibrous ring with partial prolapse of the nucleus into the spinal canal;
- the presence of acute or chronic inflammatory processes in the pathological focus (relative contraindication, sometimes ignored by doctors);
- inefficiency or development side effects after a previous operation using laser technology.
After even such a relatively safe procedure, complications are possible. In most cases, they are moderate, and do not particularly threaten the patient. But sometimes very serious consequences are possible: a recurrence of a hernia, and it can develop with renewed vigor and proceed more severely than before the operation. Moreover, the risks of this are high, since laser treatment is not a 100% method of treating intervertebral hernias.
Also, after the procedure, a pain syndrome of the type of phantom pain may develop. Its duration cannot be determined: in some people it lasts several months after the procedure, in others it can last for years.
Carrying out vaporization of a hernia of the back
In the first weeks after the operation, partial immobilization of the spinal column often develops. back to the menu
With the effectiveness of laser hernia removal, everything is not so simple: on the one hand, the procedure is safe and very effective - most patients successfully stop a hernia. On the other hand, a new hernia may develop in a few months.
What is the reason? The fact is that laser treatment is not a radical way to remove hernias (we are talking about vaporization). With its help, it is possible to partially, but not completely remove the protrusion of the nucleus pulposus, and this is precisely the problem.
In addition, too much depends on the regenerative capabilities of the body. That is, half of the success of the procedure lies not in the technique itself, but in the characteristics of the patient's body. That is why they do not prescribe treatment to people over 50 years old, since their regenerative mechanisms are too weakened. To the menu
Types of procedure
Laser treatment of hernias is divided into two types: vaporization (actually, removal of the hernia itself) and reconstruction. What are the differences between these procedures?
Laser vaporization involves the removal of an intervertebral hernia. That is, it is similar to the classic surgical operation, but it is less traumatic. During the procedure, the tissues of the nucleus pulposus are evaporated to prevent its protrusion through the annulus fibrosus.
Stages of formation of a vertebral hernia

Laser reconstruction is used to enhance the regenerative capabilities of the body (locally). The goal is simple: due to the body's ability to "heal" the intervertebral hernia. The procedure is extremely safe for the patient, but at the same time it is much lower in efficiency than vaporization. To the menu
Treatment of spinal hernia is a process that requires time, patience and professionalism of the attending physician. All treatment can be conditionally divided into the following points:
- removal of pain syndrome and reduction of swelling of tissues;
- relieve spasm of the spinal muscles;
- improvement of the nerve conduction of the spine;
- elimination of all visible signs of the inflammatory process;
- restoration of the physiological intervertebral space.
Basically, hernia treatment can be divided into: conservative, surgical and rehabilitation treatment.
Conservative treatment includes drug and non-drug therapy, which an experienced specialist will advise to use in combination. The course of drug treatment must necessarily include the appointment of such drugs:
- anti-inflammatory drugs that relieve inflammation and pain;
- muscle relaxants, which will reduce muscle spasm;
- hemorheological agents that can improve blood flow;
- the necessary painkiller for a hernia of the spine;
- vitamins of group B, which will restore the nerve conduction of the spine.
If we talk about non-drug treatment hernia, then it includes:
- such physiotherapeutic procedures as ultrasound, paraffin therapy, magnetotherapy, diadynamic currents, electrophoresis and more;
- reflexology;
- manual therapy.
Surgical treatment is prescribed if the disease is at the stage when conservative treatment no longer gives any results. Only the attending physician will be able to accurately tell the patient how to get rid of a spinal hernia.
Before deciding on the operation, the attending physician will diagnose the consequences of the intervertebral hernia, and only after that will advise the patient on one or another type of operation.
Reconstruction of vertebral discs with a laser
Removal of an intervertebral hernia with a laser demonstrates high efficiency in the treatment of young people.
Also, laser nucleoplasty of the lumbar or other spine copes well with disc protrusions up to 6 mm, it is also effective in cases where disc fragments are not separated from each other.
Treatment of spinal hernia with a laser is also used if a special endoscopic discectomy is necessary. The essence of the procedure is to introduce an endoscope and instruments through a small incision. The doctor monitors his actions through the monitor, thanks to which the hernia is gradually removed. Such an operation does not cause any particular harm to healthy tissues.
Laser discectomy does not cause complications, so scars, hematomas and adhesions do not form. The minimally invasiveness of the method allows it to be used to remove the most hernias. different sizes. The laser is often used in intraoperative coagulation of blood vessels, which avoids tissue heating, and the operation does not cause injury, so the nerve structures are not damaged.
The patient can move independently within a few hours after the operation. Reviews of patients who underwent such an operation are mostly positive. People note that the procedure was successful, without complications, and the treatment was effective.
A spinal hernia is a pathology when the fibrous ring of the intervertebral disc, in the center of which the nucleus pulposus is located, breaks due to an increase in pressure inside the disc or when a direct damaging effect is exerted. The nucleus pulposus begins to protrude outward - this condition is called a hernia.
Now reviews about the removal of the intervertebral hernia of those who were lying next to me.
Since I had gel polish on my nails, almost all the nurses of the department removed it for me with the help of alcohol and other improvised means. By the way, it was fun and at least a little distracted from anxious thoughts about the upcoming operation to remove the intervertebral hernia.
Consequences of injuries
Paresis (disfunction) of the foot;
I will remember how it all began, at the same time I will introduce you to some of the symptoms of a herniated disc of the spine.
Also, an intervertebral hernia can be triggered by excess weight. Therefore, already at the beginning of treatment, before the laser procedure, it is worth thinking about your diet. Weight should be appropriate for height and age. Thanks to its normalization, the load on the spine will decrease, and the person will feel more comfortable.
Physiotherapy
Physiotherapist, laser therapy, 25 years of experience
- Strengthening your back muscles will help you maintain a straight posture. In addition, the abdominal muscles should be developed comprehensively. Thus, the load on the spine will decrease due to its transfer to these muscles. The development of an intervertebral hernia is closely related to posture. Therefore, the disease can be prevented through regular exercise.
Massage
Specialists of the Health Workshop clinic in Moscow use laser therapy in the treatment of various diseases.
Plus, laser therapy allows, and even recommends the use and additional methods treatment: it is worth going to a massage therapist, to physiotherapy or acupuncture, to a chiropractor and other procedures that can affect the ligaments and muscles in the back. The above methods will be offered to you by a specialist of any professional clinic, because they are successfully used when laser removal of a hernia of the spine takes place.
All soft tissues in the human body are easily penetrated by directed light radiation. This means that the method by which a hernia of the spine is removed with a laser allows therapy to be carried out without even breaking the skin.
Sorry for the spelling, everyone spells this word differently on the net. That. if there is no side effect of laser VAPORIZATION, then why spend so much time and money on conservative treatment when you can fix it in an hour, of course, given the size of the hernia (up to 6mm). Thank you! Waiting for your reply.
Before I got up, I had to put on compression stockings. It was hard to come out of anesthesia. She walked only with support. It is inconvenient to walk standing up to the toilet, and also to get up from a prone position - first you need to roll over on your stomach, then get on all fours, and only after that alternately lower your legs to the floor. Frantsevna, 73 years old.
Today, the following types of surgery to remove an intervertebral hernia are most often practiced:
- I agreed to the removal of the intervertebral hernia of the lumbar.
- Every year, the pain in the lower back became more intense and appeared more often. Particularly strong pain became after the third birth. At that time I was already a little over 30, my daughter was 3 months old. One morning, the pain became so severe that I could not even take a step, get out of bed. The only forced position of the body, in which the pain was more or less tolerable, was sitting. I did not have the opportunity to do an MRI to establish an accurate diagnosis of my disease at that time. I took painkillers and underwent a course of reflex magnetic relaxation of the spine. It became much easier for me, the pain receded, and I even forgot how unbearably my back can hurt. I encountered other symptoms of an intervertebral hernia after 3 years.
- As for swimming, two to three months after a procedure such as laser treatment of the spine, going to the pool will be a great way not only to strengthen the spinal muscles, but also give you the opportunity to constantly develop it. It is generally recommended to swim at least 2 times a week. The average duration of classes is 50 minutes. In general, it does not matter what style a person will swim in, but if he has problems with the cervical region, then it is best to swim on his back.
Gymnastics.
How to start living without pain and worries
- Laser therapy helps with osteochondrosis, intervertebral hernia, protrusion of the intervertebral discs. Due to diseases of the musculoskeletal system, a person quickly gets tired, may feel numbness in the arms and legs. Thanks to the procedure, stiffness in movements, pain in the back, neck, lower back, and chest disappear. Laser treatment reduces swelling and the size of the herniated spine.
- But the procedure of laser reconstruction has an effect only in relation to the root cause of the disease - it puts in order damage to the intervertebral discs. Those who preferred the removal of a hernia of the spine with a laser agree on one thing - complex therapy leads you to the fastest and most comfortable return to normal life.
- A beam of laser beams affects the affected area, the temperature increases pointwise, “evaporating” the damaged area of the disc. For each, a special treatment is selected with a certain type of nozzle, which ensures the achievement of the most effective procedure.
- Any self-respecting surgeon will say that where you can do without surgery, it is better to carry out conservative treatment. But there are many cases where surgical treatment is the method of choice, unfortunate healers promise to cure the patient without surgery. The healers' wallets are getting fat, but the operation still has to be done.
Immediately after the operation, the pain was gone. She straightened up and began to walk straight. It didn't hurt anywhere. Now (a month has passed since the operation) sometimes he shoots in the buttock. Very worried question intimate life. They said that you can carefully in a month and a half. Anya, 31
Discectomy;
This disease can manifest itself at any age. Although the sources indicate that the "age of the hernia" is approximately 30 - 55 years. After 25 years, the spine “ages”, and without prevention, the risk of disease increases.
- Lower back pain began to appear very often - after any physical activity. I picked up my daughter - my back hurts, I did fitness - it shoots in my lower back, I sat at the computer for a long time - I can hardly straighten up.
- In addition, with a hernia of the spine, it is necessary to quit smoking. The fact is that as a result of this bad habit, the vessels are greatly narrowed and thus do not allow the intervertebral discs to receive all the necessary components. The same goes for alcohol. Subsequently, moderate alcohol consumption and smoking cessation will also prevent the appearance of a hernia.
- Any of these procedures will have a beneficial effect on the back muscles, significantly strengthen them. Moreover, such treatment can be continued both in the same clinic where the laser operation was performed, and in other medical institutions. The task of complex treatment consists in two important stages, which are interconnected. Laser herniation removal, also called laser vaporization of herniated discs, is just about removing the root cause. And the subsequent recovery with the help of the complex is also the prevention of this problem.
Fill out an application on the website
Laser therapy is effective for sciatica, neuritis, neuralgia, nervous tics. Due to diseases nervous system appears headache, dizziness, nausea, tinnitus, fainting, worsening memory. The patient feels weakness in the arms and legs, he may have problems sleeping.
After the patient has undergone the removal of a vertebral hernia with a laser, physiotherapy exercises can be especially useful. It allows you to form a strengthened muscular frame on the back, which will exclude the recurrence and progression of degenerative changes, this will protect other parts of the spine.
In addition, exposure to temperature stimulates the process of regeneration and renewal of cartilage tissues. At the time of the operation, the patient is conscious - this makes it possible to track the progress of the procedure on the monitor.
- Fedya said: Sorry for the spelling, everyone writes this word differently on the net. That. if there is no side effect of laser VAPORIZATION, then why spend so much time and money on conservative treatment when you can fix it in an hour, of course, given the size of the hernia (up to 6mm). Thank you! Waiting for your reply.Click to expand...The operation has effectiveness and side effects. The efficiency of this type of operation, with a disc herniation of up to 6 mm and without rupture of the fibrous ring, is 60-70% (I don’t give a link, it’s possible on this forum, colleagues will correct the figure). Side effects, of course possible, up to death. Only with this type there are fewer of them.
- My leg didn't hurt after the surgery. The doctors said that this was within the normal range - the root was pinched for a long time and there was swelling. After the operation, you can sleep on your back, on your stomach, and on your sides. I was scared that I would only need to lie on my stomach. After the operation, you can not sit for a month and a half and you need to wear a corset for the same amount. Of course, physical activity is limited. Sick leave for 60 days is also given. Sveta, 35 years old
- microdiscectomy;
- And after 55, the intervertebral discs are less mobile, so the risk of a hernia is reduced.
- Over time, the pain began to spread to the leg. You know, that feeling when you shoot in the back and give it to the leg. The pain was tolerable, but very frequent.
You are tormented by discomfort at the site of the protrusion of the hernia ...
Preparing a patient for laser removal of a vertebral hernia
Before removal, basic preparation is carried out, which does not require any specific actions. The basis of all preparation is an attempt to exclude the presence of contraindications in the patient. In addition, the nuances of the course of the intervertebral hernia are revealed, which makes it much more efficient and safer to perform the operation.
Preparation for this treatment includes:
- Examination of the patient by a neurosurgeon.
- Taking x-rays and/or computed tomography(less commonly used magnetic resonance imaging).
- Taking an electrocardiogram of the heart.
- Biochemical analyzes blood and urine.
Laser treatment of vertebral hernia
You may also need to consult with a therapist and an anesthesiologist (especially if general anesthesia will be performed). The last meal should be 10 hours before the procedure.to the menu
Treatment of spinal hernia with a laser is indicated for patients with pathologies at an early stage, when there is still the possibility of recovery without a radical approach. Laser irradiation of the intervertebral hernia is also the final step in the removal of discs, which allows you to speed up the restoration of spinal tissues and shorten the rehabilitation period. Laser vaporization for hernia, as reviews show, is effective for patients different ages except for people with contraindications.
Immediately after the laser vaporization, the patient feels better, the pain syndrome stops, and the stiffness of movements disappears. Under the influence of the laser, cellular structures begin to recover, which takes place several months after the procedure.
Treatment of a hernia of the spine with a laser leaves no traces after the operation, the patient can return to normal life already on the first day after the operation to remove the protrusion. Laser disc removal eliminates the risk of postoperative complications and recurrence of the disease, in addition, the operation does not require anesthesia, so this treatment is ideal for people who are intolerant to pain relief.
Conduct method
Removal of residual tissues after disc removal surgery is carried out by irradiating the operating area as the final stage of treatment. But laser vaporization refers to independent methods of treating intervertebral pathology. The intensity of irradiation is optimal for partial evaporation of the liquid, but cartilage tissue does not collapse, during which the disk gradually falls into place.
Removal of excess fluid leads to the reverse development of the disease, the defect returns to the disc body. Before starting the procedure, local anesthesia tissue at the site of needle insertion, and the entire procedure is controlled by a CT scanner.
- The operation is performed under local anesthesia, there is no need for general anesthesia.
- The needle pierces the intervertebral disc by 2 cm.
- A quartz fiber light guide is inserted through the needle.
- There is a laser effect on the disk.
An improvement in the patient's condition is observed already at the time of the procedure, when the fluid is removed. This is confirmed by the reviews of patients who have undergone treatment of intervertebral hernia with a laser. Surgery for lesions of the cervical spine is most effective, recovery occurs within a few weeks after the procedure.
Contraindications
Laser vaporization is not carried out in such cases:
- acute inflammation in the spine;
- tumor of any localization;
- period of pregnancy;
- toxic poisoning, nervous overexcitation, mental illness;
- acute or chronic infections.
Compliance with safety measures, and the right operation will be an effective option for the treatment of vertebral hernia with a minimal risk of recurrence (0.2%).