Antipyretics for children are prescribed by a pediatrician. But there are emergency situations for fever when the child needs to be given medicine immediately. Then the parents take responsibility and use antipyretic drugs. What is allowed to be given to infants? How can you lower the temperature in older children? What medications are the safest?
Questions that arise while reading the article can be asked to specialists using the online form.
Free consultations are available 24 hours a day.
What is an ECG?
Electrocardiography is a method used to record electrical currents that occur during contractions and relaxations of the heart muscle. An electrocardiograph is used to conduct the study. Using this device, it is possible to record electrical impulses that come from the heart and convert them into a graphic drawing. This image is called an electrocardiogram.
Electrocardiography reveals disturbances in the functioning of the heart and disruptions in the functioning of the myocardium. In addition, after decoding the results of the electrocardiogram, some non-cardiac diseases can be detected.
How does an electrocardiograph work?
The electrocardiograph consists of a galvanometer, amplifiers and a recorder. Weak electrical impulses that arise in the heart are read by electrodes and then amplified. The galvanometer then receives data on the nature of the pulses and transmits them to the recorder. In the recorder, graphic images are printed on special paper. The graphs are called cardiograms.
How is an EKG done?
Electrocardiography is performed according to established rules. Below is the procedure for taking an ECG:
Many of our readers actively use a well-known method based on natural ingredients, discovered by Elena Malysheva, to treat HEART DISEASES. We recommend that you check it out.
- The person removes metal jewelry, removes clothing from the legs and upper body, and then assumes a horizontal position.
- The doctor treats the contact points between the electrodes and the skin, and then places the electrodes in certain places on the body. Next, he fixes the electrodes on the body with clips, suction cups and bracelets.
- The doctor attaches the electrodes to the cardiograph, after which the impulses are recorded.
- A cardiogram is recorded, which is the result of electrocardiography.
Separately, it should be said about the leads used for ECG. The following leads are used:
- 3 standard leads: one of them is located between the right and left arms, the second – between the left leg and right arm, the third – between the left leg and left arm.
- 3 limb leads with enhanced character.
- 6 leads located on the chest.
In addition, additional leads can be used if necessary.
After the cardiogram is recorded, it is necessary to decrypt it. This will be discussed further.
Deciphering the cardiogram
Conclusions about diseases are made on the basis of heart parameters obtained after deciphering the cardiogram. The following is the procedure for decoding the ECG:
- The heart rhythm and myocardial conduction are analyzed. To do this, the regularity of contractions of the heart muscle and the frequency of myocardial contractions are assessed, and the source of excitation is determined.
- The regularity of heart contractions is determined as follows: the R-R intervals between successive cardiac cycles are measured. If the measured R-R intervals are the same, then a conclusion is made about the regularity of contractions of the heart muscle. If the duration of the R-R intervals is different, then a conclusion is drawn about the irregularity of heart contractions. If a person exhibits irregular contractions of the myocardium, then a conclusion is drawn about the presence of arrhythmia.
- The heart rate is determined by a certain formula. If a person’s heart rate exceeds the norm, then a conclusion is drawn about the presence of tachycardia, but if a person’s heart rate is below normal, then a conclusion is drawn about the presence of bradycardia.
- The point from which the excitation comes is determined as follows: the movement of contraction in the cavities of the atria is assessed and the relationship of the R waves to the ventricles is established (according to the QRS complex). The nature of the heart rhythm depends on the source that causes the excitation.
The following patterns of heart rhythms are observed:
- The sinusoidal nature of the heart rhythm, in which the P waves in the second lead are positive and are in front of the ventricular QRS complex, and the P waves in the same lead have an indistinguishable shape.
- Atrial rhythm of the nature of the heart, in which the P waves in the second and third leads are negative and are in front of the unchanged QRS complexes.
- The ventricular nature of the heart rhythm, in which there is a deformation of the QRS complexes and a loss of communication between the QRS (complex) and the P waves.
Cardiac conductivity is determined as follows:
- Measurements of P wave length, PQ interval length, and QRS complex are assessed. Exceeding the normal duration of the PQ interval indicates too low conduction velocity in the corresponding cardiac conduction section.
- The rotations of the myocardium around the longitudinal, transverse, anterior and rear axles. For this purpose, the position is assessed electrical axis heart in a common plane, after which the presence of turns of the heart along one axis or another is established.
- The atrial P wave is analyzed. For this, the amplitude of the P bison is assessed, the duration of the P wave is measured. After that, the shape and polarity of the P wave are determined.
- The ventricular complex is analyzed - For this, the QRS complex, the RS-T segment, the QT interval, the T wave are evaluated.
During the assessment of the QRS complex, do the following: determine the characteristics of the Q, S and R waves, compare the amplitude values of the Q, S and R waves in a similar lead and the amplitude values of the R/R waves in different leads.
Having carefully studied the methods of Elena Malysheva in the treatment of tachycardia, arrhythmia, heart failure, stena cordia and general healing of the body, we decided to bring it to your attention.
At the time of evaluation of the RS-T segment, the nature of the displacement of the RS-T segment is determined. The displacement can be horizontal, oblique and oblique.
During the period of analysis of the T wave, the nature of the polarity, amplitude and shape are determined. The QT interval is measured by the time from the beginning of the QRT complex to the end of the T wave. When assessing the QT interval, do the following: analyze the interval from the starting point of the QRS complex to the end point of the T wave. To calculate the QT interval, the Bezzet formula is used: the QT interval is equal to the product R-R interval and a constant coefficient.
The coefficient for QT depends on gender. For men, the constant coefficient is 0.37, and for women – 0.4.
A conclusion is made and the results are summed up.
In conclusion, the ECG specialist draws conclusions about the frequency of the contractile function of the myocardium and heart muscle, as well as the source of excitation and the nature of the heart rhythm and other indicators. In addition, an example of the description and characteristics of the P wave, QRS complex, RS-T segment, QT interval, T wave is given.
Based on the conclusion, it is concluded that a person has heart disease or other ailments of internal organs.
Electrocardiogram norms
The table with ECG results has a visual appearance, consisting of rows and columns. In the 1st column, the lines list: heart rate, beat rate examples, QT intervals, examples of axis displacement characteristics, P-wave readings, PQ readings, QRS reading examples. ECG is carried out equally in adults, children and pregnant women, but the norm is different.
The ECG norm for adults is presented below:
- heart rate in a healthy adult: sinus;
- P wave index in a healthy adult: 0.1;
- the frequency of contractions of the heart muscle in a healthy adult: 60 beats per minute;
- QRS indicator in a healthy adult: from 0.06 to 0.1;
- QT score in a healthy adult: 0.4 or less;
- RR in a healthy adult: 0.6.
In the case of observation of deviations from the norm in an adult, a conclusion is made about the presence of the disease.
The norms of cardiogram indicators in children are presented below:
- P wave index in a healthy child: 0.1 or less;
- heart rate in a healthy child: 110 beats per minute or less in children under 3 years old, 100 beats per minute or less in children under 5 years old, no more than 90 beats per minute in children in adolescence;
- QRS indicator in all children: from 0.06 to 0.1;
- QT score in all children: 0.4 or less;
- PQ in all children: if the child is under 14 years old, then the example PQ is 0.16, if the child is from 14 to 17 years old, then the PQ is 0.18, after 17 years the normal PQ is 0.2.
If in children, when deciphering the ECG, any deviations from the norm were found, then treatment should not be started immediately. Some heart problems improve with age in children.
But in children, heart disease can also be congenital. It is possible to determine whether a newborn child will have a heart pathology even at the stage of fetal development. For this purpose, electrocardiography is performed on women during pregnancy.
The norm of electrocardiogram indicators in women during pregnancy is presented below:
- heart rate in a healthy adult child: sinus;
- P wave indicator for everyone healthy women during pregnancy: 0.1 or less;
- heart muscle contraction frequency in all healthy women during pregnancy: 110 or less beats per minute in children under 3 years of age, 100 or less beats per minute in children under 5 years of age, no more than 90 beats per minute in adolescent children;
- QRS indicator for all expectant mothers during pregnancy: from 0.06 to 0.1;
- QT index in all expectant mothers during pregnancy: 0.4 or less;
- PQ indicator for all expectant mothers during pregnancy: 0.2.
It is worth noting that during different periods of pregnancy, ECG readings may differ slightly. In addition, it should be noted that performing an ECG during pregnancy is safe for both the woman and the developing fetus.
Additionally
It is worth saying that under certain circumstances, electrocardiography can give an inaccurate picture of a person’s health status.
If, for example, a person subjected himself to heavy physical activity before an ECG, then when deciphering the cardiogram, an erroneous picture may be revealed.
This is explained by the fact that during physical activity the heart begins to work differently than at rest. During physical activity, the heart rate increases, and some changes in the rhythm of the myocardium may be observed, which is not observed at rest.
It is worth noting that the work of the myocardium is affected not only by physical stress, but also by emotional stress. Emotional stress, like physical stress, disrupts the normal course of myocardial function.
At rest, the heart rhythm normalizes and the heartbeat evens out, so before electrocardiography you must be at rest for at least 15 minutes.
- Do you often have discomfort in the area of the heart (stabbing or squeezing pain, burning sensation)?
- You may suddenly feel weak and tired.
- The pressure is constantly fluctuating.
- There is nothing to say about shortness of breath after the slightest physical exertion...
- And you have been taking a bunch of medications for a long time, going on a diet and watching your weight.
Interpretation of ECG in adults and children, norms in tables and other useful information
Pathology of cardio-vascular system is one of the most common problems that affects people of all ages. Timely treatment and diagnosing the functioning of the circulatory system can significantly reduce the risk of developing dangerous diseases.
Today, the most effective and easily accessible method for studying heart function is an electrocardiogram.
Basic Rules
When studying the results of a patient’s examination, doctors pay attention to such components of the ECG as:
There are strict normal parameters for each line on the ECG tape, the slightest deviation from which may indicate disturbances in the functioning of the heart.
Cardiogram analysis
The entire set of ECG lines is examined and measured mathematically, after which the doctor can determine some parameters of the work of the heart muscle and its conduction system: heart rhythm, heart rate, pacemaker, conductivity, electrical axis of the heart.
Today, all these indicators are studied by high-precision electrocardiographs.
Sinus rhythm of the heart
This is a parameter that reflects the rhythm of heart contractions that occur under the influence of the sinus node (normal). It shows the coherence of the work of all parts of the heart, the sequence of processes of tension and relaxation of the heart muscle.
The rhythm is very easy to determine by the highest R waves: if the distance between them is the same throughout the entire recording or deviates by no more than 10%, then the patient does not suffer from arrhythmia.
The number of beats per minute can be determined not only by counting the pulse, but also by ECG. To do this, you need to know the speed at which the ECG was recorded (usually 25, 50 or 100 mm/s), as well as the distance between the highest teeth (from one vertex to another).
By multiplying the recording duration of one mm by the length of the R-R segment, you can get the heart rate. Normally, its performance ranges from 60 to 80 beats per minute.
Excitation source
The autonomic nervous system of the heart is designed in such a way that the contraction process depends on the accumulation of nerve cells in one of the zones of the heart. Normally, this is the sinus node, impulses from which disperse throughout the nervous system of the heart.
In some cases, the role of pacemaker can be taken over by other nodes (atrial, ventricular, atrioventricular). This can be determined by examining the P wave - inconspicuous, located just above the isoline.
What is postmyocardial cardiosclerosis and why is it dangerous? Is it possible to cure it quickly and effectively? Are you at risk? Find out everything!
The causes of the development of cardiac cardiosclerosis and the main risk factors are discussed in detail in our next article.
You can read detailed and comprehensive information about the symptoms of cardiac cardiosclerosis here.
Conductivity
This is a criterion showing the process of momentum transfer. Normally, impulses are transmitted sequentially from one pacemaker to another, without changing the order.
Electric axis
An indicator based on the process of ventricular excitation. Mathematical analysis of the Q, R, S waves in leads I and III allows us to calculate a certain resulting vector of their excitation. This is necessary to establish the functioning of the branches of the His bundle.
The resulting angle of inclination of the heart axis is estimated by its value: 50-70° normal, 70-90° deviation to the right, 50-0° deviation to the left.
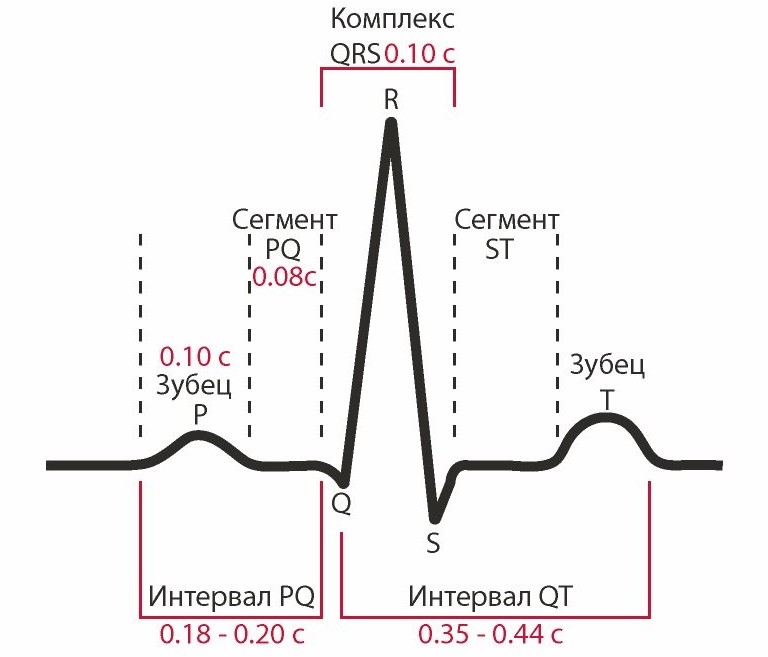
Teeth, segments and intervals
Waves are sections of the ECG lying above the isoline, their meaning is as follows:
- P – reflects the processes of contraction and relaxation of the atria.
- Q, S – reflect the processes of excitation of the interventricular septum.
- R – process of ventricular excitation.
- T – process of relaxation of the ventricles.
Intervals are ECG sections lying on the isoline.
- PQ – reflects the propagation time of the impulse from the atria to the ventricles.
Segments are sections of an ECG, including an interval and a wave.
- QRST – duration of ventricular contraction.
- ST – time of complete excitation of the ventricles.
- TP – time of electrical diastole of the heart.
Normal for men and women
Decoding ECG of the heart and norms of indicators in adults are presented in this table:
Healthy Childhood Outcomes
Interpretation of the results of ECG measurements in children and their norm in this table:
Dangerous diagnoses
Which dangerous conditions can it be determined by ECG readings during decoding?
Extrasystole
This phenomenon is characterized by an abnormal heart rhythm. The person feels a temporary increase in contraction frequency followed by a pause. It is associated with the activation of other pacemakers, which, along with the sinus node, send an additional volley of impulses, which leads to an extraordinary contraction.
Arrhythmia
It is characterized by a change in the periodicity of sinus rhythm, when impulses arrive at different frequencies. Only 30% of such arrhythmias require treatment, because can provoke more serious diseases.
In other cases, this may be a manifestation physical activity, change hormonal levels, the result of a previous fever and does not threaten health.
Bradycardia
It occurs when the sinus node is weakened, unable to generate impulses with the proper frequency, as a result of which the heart rate slows down, down to beats per minute.
Tachycardia
The opposite phenomenon, characterized by an increase in heart rate of more than 90 beats per minute. In some cases, temporary tachycardia occurs under the influence of severe physical exertion and emotional stress, as well as during illnesses associated with increased temperature.
Conduction disturbance
In addition to the sinus node, there are other underlying pacemakers of the second and third orders. Normally, they conduct impulses from the first-order pacemaker. But if their functions weaken, a person may feel weakness and dizziness caused by depression of the heart.
It is also possible to downgrade blood pressure, because the ventricles will contract less frequently or arrhythmically.
Why there might be differences in performance
In some cases, when re-analyzing the ECG, deviations from previously obtained results are revealed. With what it can be connected?
- Different times of the day. Typically, an ECG is recommended to be done in the morning or afternoon, when the body has not yet been exposed to stress factors.
- Loads. It is very important that the patient is calm while recording the ECG. The release of hormones can increase heart rate and distort performance. In addition, it is also not recommended to engage in heavy physical labor before the examination.
- Eating. Digestive processes affect blood circulation, and alcohol, tobacco and caffeine can affect heart rate and blood pressure.
- Electrodes. Incorrect application or accidental displacement can seriously change the indicators. Therefore, it is important not to move during recording and to degrease the skin in the area where the electrodes are applied (the use of creams and other skin products before the examination is highly undesirable).
- Background. Sometimes other devices can interfere with the operation of the electrocardiograph.
Find out everything about recovery after a heart attack - how to live, what to eat and what to treat to support your heart?
Is there a disability category after a heart attack and what can you expect in terms of work? We will tell in our review.
Rare but accurate myocardial infarction of the posterior wall of the left ventricle - what is it and why is it dangerous?
Additional examination methods
Holter
A method of long-term study of heart function, possible thanks to a portable compact tape recorder that is capable of recording the results on magnetic film. The method is especially good when it is necessary to study periodically occurring pathologies, their frequency and time of appearance.
Treadmill
Unlike a conventional ECG, which is recorded at rest, this method is based on the analysis of results after physical activity. Most often, this is used to assess the risk of possible pathologies not detected on a standard ECG, as well as when prescribing a course of rehabilitation for patients who have suffered a heart attack.
Phonocardiography
Allows you to analyze heart sounds and murmurs. Their duration, frequency and time of occurrence correlate with the phases of cardiac activity, which makes it possible to assess the functioning of the valves and the risks of developing endo- and rheumatic carditis.
A standard ECG is a graphical representation of the work of all parts of the heart. Many factors can affect its accuracy, so you should follow your doctor's recommendations.
The examination reveals most pathologies of the cardiovascular system, but additional tests may be required for an accurate diagnosis.
Finally, we suggest watching a video course on decoding “An ECG can be done by everyone”:
Decoding a cardiogram in children and adults: general principles, reading the results, an example of decoding
Definition and essence of the method
How to correctly perform an electrocardiogram followed by
The principle of decoding an ECG
ECG interpretation plan - general scheme for reading results
- position of the electrical axis of the heart;
- determining the correctness of the heart rhythm and conductivity of the electrical impulse (blockades, arrhythmias are identified);
- determining the regularity of contractions of the heart muscle;
- determination of heart rate;
- identifying the source of the electrical impulse (whether sinus rhythm is determined or not);
- analysis of the duration, depth and width of the atrial P wave and the P – Q interval;
- analysis of the duration, depth, width of the QRST ventricular wave complex;
- analysis of parameters of the RS – T segment and T wave;
- analysis of Q – T interval parameters.
Based on all the studied parameters, the doctor writes a final conclusion on the electrocardiogram. The conclusion may roughly look like this: “Sinus rhythm with heart rate 65. Normal position of the electrical axis of the heart. No pathology was detected." Or this: “Sinus tachycardia with heart rate 100. Single supraventricular extrasystole. Incomplete blockade of the right bundle branch. Moderate metabolic changes in the myocardium."
- sinus rhythm or not;
- rhythm regularity;
- heart rate (HR);
- position of the electrical axis of the heart.
If any of the 4 are identified pathological syndromes, then indicate which ones - disturbance of rhythm, conduction, overload of the ventricles or atria, and damage to the structure of the heart muscle (infarction, scar, dystrophy).
Example of deciphering an electrocardiogram
Checking the regularity of heart contractions
Heart rate (HR) calculation
1. The speed of the tape is 50 mm/s - then the heart rate is 600 divided by the number of squares.
2. The speed of the tape is 25 mm/s - then the heart rate is 300 divided by the number of squares.
Identifying the source of the rhythm
Decoding ECG - rhythms
Detection of pathology of electrical impulse conduction through the structures of the heart
Electrical axis of the heart
Atrial P wave
- positive in I, II, aVF and chest leads (2, 3,4, 5, 6);
- negative in aVR;
- biphasic (part of the tooth lies in the positive region, and part in the negative) in III, aVL, V1.
The normal duration of P is no more than 0.1 seconds, and the amplitude is 1.5 - 2.5 mm.
1. Tall and sharp teeth in leads II, III, aVF appear with hypertrophy of the right atrium (“cor pulmonale”);
2. A P wave with two peaks and a large width in leads I, aVL, V5 and V6 indicates hypertrophy of the left atrium (for example, mitral valve disease).
P–Q interval
- I degree: simple lengthening of the P–Q interval while preserving all other complexes and waves.
- II degree: prolongation of the P–Q interval with partial loss of some QRS complexes.
- III degree: lack of connection between the P wave and QRS complexes. In this case, the atria work in their own rhythm, and the ventricles - in their own.
Ventricular QRST complex
T wave
Q-T interval
ECG interpretation - normal indicators
5. Heart rate is 70 – 75 beats per minute.
6. sinus rhythm.
7. The electrical axis of the heart is located normally.
Interpretation of ECG in children and pregnant women
Decoding the electrocardiogram during a heart attack
The most acute stage of myocardial infarction can last for 3 hours - 3 days from the moment of circulatory disturbance. At this stage, the Q wave may be absent on the electrocardiogram. If it is present, then the R wave has a low amplitude or is completely absent. In this case, there is a characteristic QS wave, reflecting a transmural infarction. The second sign of an acute infarction is an increase in the S-T segment by at least 4 mm above the isoline, with the formation of one large T wave.
Interpretation of the most common ECGs
Also, myocardial hypertrophy can be a consequence of previous heart attacks.
What is an ECG, how to decipher it yourself
From this article you will learn about such a diagnostic method as an ECG of the heart - what it is and what it shows. How an electrocardiogram is recorded, and who can most accurately decipher it. You will also learn how to independently determine the signs of a normal ECG and major heart diseases that can be diagnosed using this method.
What is an ECG (electrocardiogram)? This is one of the simplest, most accessible and informative methods for diagnosing heart disease. It is based on recording electrical impulses arising in the heart and graphically recording them in the form of teeth on a special paper film.
Based on these data, one can judge not only the electrical activity of the heart, but also the structure of the myocardium. This means that using an ECG you can diagnose many various diseases hearts. Therefore, independent interpretation of the ECG by a person who does not have special medical knowledge is impossible.
All that an ordinary person can do is only roughly assess the individual parameters of the electrocardiogram, whether they correspond to the norm and what pathology they may indicate. But final conclusions based on the ECG conclusion can only be made by a qualified specialist - a cardiologist, as well as a therapist or family doctor.
Principle of the method
The contractile activity and functioning of the heart is possible due to the fact that spontaneous electrical impulses (discharges) regularly occur in it. Normally, their source is located in the uppermost part of the organ (in the sinus node, located near the right atrium). The purpose of each impulse is to travel along the nerve pathways through all parts of the myocardium, causing them to contract. When an impulse arises and passes through the myocardium of the atria and then the ventricles, their alternating contraction occurs - systole. During the period when there are no impulses, the heart relaxes - diastole.
ECG diagnostics (electrocardiography) is based on recording electrical impulses arising in the heart. For this purpose, a special device is used - an electrocardiograph. The principle of its operation is to capture on the surface of the body the difference in bioelectric potentials (discharges) that occur in different parts of the heart at the moment of contraction (in systole) and relaxation (in diastole). All these processes are recorded on special heat-sensitive paper in the form of a graph consisting of pointed or hemispherical teeth and horizontal lines in the form of spaces between them.
What else is important to know about electrocardiography
Electrical discharges of the heart pass not only through this organ. Since the body has good electrical conductivity, the strength of the exciting cardiac impulses is sufficient to pass through all tissues of the body. They spread best to the chest in the area where the heart is located, as well as to the upper and lower limbs. This feature is the basis of the ECG and explains what it is.
In order to record the electrical activity of the heart, it is necessary to fix one electrocardiograph electrode on the arms and legs, as well as on the anterolateral surface of the left half chest. This allows you to capture all directions of electrical impulses propagating throughout the body. The paths of discharges between the areas of contraction and relaxation of the myocardium are called cardiac leads and are designated on the cardiogram as follows:
- Standard leads:
- I – first;
- II – second;
- Ш – third;
- AVL (similar to the first);
- AVF (analogue of the third);
- AVR (mirroring all leads).
- Chest leads (different points on the left side of the chest, located in the heart area):
The significance of the leads is that each of them registers the passage of an electrical impulse through a certain area of the heart. Thanks to this, you can obtain information about:
- How the heart is located in the chest (the electrical axis of the heart, which coincides with the anatomical axis).
- What is the structure, thickness and nature of blood circulation of the myocardium of the atria and ventricles.
- How regularly do impulses occur in the sinus node and are there any interruptions?
- Are all impulses carried out along the paths of the conducting system, and are there any obstacles in their path?
What does an electrocardiogram consist of?
If the heart had the same structure of all its departments, nerve impulses would pass through them in the same time. As a result, on the ECG, each electrical discharge would correspond to only one tooth, which reflects the contraction. The period between contractions (impulses) on the EGC looks like an even horizontal line, which is called an isoline.
The human heart consists of right and left halves, in which the upper part is the atria, and the lower part is the ventricles. Because they have different sizes, thickness and separated by partitions, exciting impulse with at different speeds passes through them. Therefore, different waves corresponding to a specific part of the heart are recorded on the ECG.
What do the teeth mean?
The sequence of propagation of systolic excitation of the heart is as follows:
- The origin of electric pulse discharges occurs in the sinus node. Since it is located close to the right atrium, it is this section that contracts first. With a slight delay, almost simultaneously, the left atrium contracts. On the ECG, such a moment is reflected by the P wave, which is why it is called atrial. It faces up.
- From the atria, the discharge passes to the ventricles through the atrioventricular (atrioventricular) node (a collection of modified myocardial nerve cells). They have good electrical conductivity, so delays in the node do not normally occur. This is displayed on the ECG as the P-Q interval - a horizontal line between the corresponding teeth.
- Excitation of the ventricles. This part of the heart has the thickest myocardium, so the electrical wave travels through them longer than through the atria. As a result, the highest wave appears on the ECG - R (ventricular), facing upward. It may be preceded by a small Q wave, the apex of which faces in the opposite direction.
- After the completion of ventricular systole, the myocardium begins to relax and restore energy potentials. On the ECG it looks like an S wave (facing down) - a complete lack of excitability. After it comes a small T wave, facing upward, preceded by a short horizontal line - the S-T segment. They indicate that the myocardium has fully recovered and is ready to make another contraction.
Since each electrode attached to the limbs and chest (lead) corresponds to a specific part of the heart, the same teeth look different in different leads - they are more pronounced in some, and less in others.
How to decipher a cardiogram
Sequential ECG interpretation in both adults and children involves measuring the size, length of the waves and intervals, assessing their shape and direction. Your actions with decryption should be as follows:
- Unfold the paper with the recorded ECG. It can be either narrow (about 10 cm) or wide (about 20 cm). You will see several jagged lines running horizontally, parallel to each other. After a short interval in which there are no teeth, after the recording is interrupted (1–2 cm), the line with several complexes of teeth begins again. Each such graph displays a lead, so it is preceded by a designation of which lead it is (for example, I, II, III, AVL, V1, etc.).
- In one of the standard leads (I, II or III) in which the R wave is the highest (usually the second), measure the distance between three successive R waves (R-R-R interval) and determine the average value (divide number of millimeters per 2). This is necessary to calculate the heart rate per minute. Remember that these and other measurements can be made with a millimeter ruler or by calculating the distance using an ECG tape. Each large cell on the paper corresponds to 5 mm, and each dot or small cell inside it corresponds to 1 mm.
- Assess the spaces between the R waves: are they the same or different? This is necessary in order to determine the regularity of the heart rhythm.
- Sequentially evaluate and measure each wave and interval on the ECG. Determine their compliance with normal indicators (table below).
Important to remember! Always pay attention to the speed of the tape - 25 or 50 mm per second. This is fundamentally important for calculating heart rate (HR). Modern devices indicate heart rate on a tape, and there is no need to count.
How to calculate the heart rate
There are several ways to count the number of heartbeats per minute:
- Typically, the ECG is recorded at a speed of 50 mm/sec. In this case, you can calculate your heart rate (heart rate) using the following formulas:
What does an ECG look like normally and with pathology?
What a normal ECG and wave complexes should look like, what deviations occur most often and what they indicate are described in the table.
Electrocardiography is one of the most common and most informative methods for diagnosing a huge number of diseases. An ECG involves a graphical display of the electrical potentials that are formed in the beating heart. Indicators are taken and displayed using special devices - electrocardiographs, which are constantly being improved.
Table of contents:As a rule, during the study, 5 waves are recorded: P, Q, R, S, T. In some moments, it is possible to record a subtle U wave.

Electrocardiography allows you to identify the following indicators, as well as variants of deviations from reference values:
- Heart rate (pulse) and regularity of myocardial contractions (arrhythmias and extrasystoles can be detected);
- Disturbances in the heart muscle of an acute or chronic nature (in particular, with ischemia or heart attack);
- metabolic disorders of the main compounds with electrolytic activity (K, Ca, Mg);
- intracardiac conduction disorders;
- hypertrophy of the heart (atria and ventricles).
 Note:when used in parallel with a cardiophone, the electrocardiograph makes it possible to remotely determine some acute diseases heart (presence of areas of ischemia or infarction).
Note:when used in parallel with a cardiophone, the electrocardiograph makes it possible to remotely determine some acute diseases heart (presence of areas of ischemia or infarction).
ECG is the most important screening technique for detecting coronary artery disease. Valuable information is provided by electrocardiography with the so-called. "stress tests".
Isolated or in combination with other diagnostic techniques, ECG is often used in the study of cognitive (thought) processes.
Important:An electrocardiogram must be taken during medical examination, regardless of age and general condition patient.
We recommend reading:ECG: indications for performance
There are a number of pathologies of the cardiovascular system and other organs and systems for which electrocardiographic examination is prescribed. These include:
- angina pectoris;
- myocardial infarction;
- reactive arthritis;
- peri- and myocarditis;
- periarteritis nodosa;
- arrhythmias;
- acute renal failure;
- diabetic nephropathy;
- scleroderma.
With right ventricular hypertrophy, the amplitude of the S wave in leads V1-V3 increases, which may be an indicator of symmetric pathology on the part of the left ventricle.

With left ventricular hypertrophy, the R wave is pronounced in the left precordial leads and its depth is increased in leads V1-V2. The electrical axis is either horizontal or deviated to the left, but can often correspond to the norm. The QRS complex in lead V6 is characterized by a qR or R shape.
Note:This pathology is often accompanied by secondary changes in the heart muscle (dystrophy).
Left atrial hypertrophy is characterized by a fairly significant increase in the P wave (up to 0.11-0.14 s). It acquires a “two-humped” shape in the left chest leads and leads I and II. In rare clinical cases, some flattening of the wave is noted, and the duration of the internal deviation of P exceeds 0.06 s in leads I, II, V6. Among the most prognostically reliable evidence of this pathology is an increase in the negative phase of the P wave in lead V1.
Hypertrophy of the right atrium is characterized by an increase in the amplitude of the P wave (over 1.8-2.5 mm) in leads II, III, aVF. This tooth acquires a characteristic pointed shape, and the electrical axis P is installed vertically or has a slight shift to the right.
Combined atrial hypertrophy is characterized by parallel expansion of the P wave and an increase in its amplitude. In some clinical cases, changes such as sharpening of P in leads II, III, aVF and splitting of the apex in I, V5, V6 are noted. In lead V1, an increase in both phases of the P wave is occasionally recorded.

For heart defects formed during intrauterine development, a significant increase in the amplitude of the P wave in leads V1-V3 is more common.
In patients with a severe form of chronic pulmonary heart disease with emphysematous lung damage, as a rule, an S-type ECG is determined.
Important:combined hypertrophy of two ventricles at once is rarely detected by electrocardiography, especially if the hypertrophy is uniform. In this case, the pathological signs tend to compensate each other.
With “premature ventricular excitation syndrome” on the ECG, the width of the QRS complex increases and the PR interval becomes shorter. The delta wave, which affects the increase in the QRS complex, is formed as a result of an early increase in the activity of areas of the cardiac muscle of the ventricles.
Blockades are caused by the cessation of the electrical impulse in one of the areas.

Impairments in impulse conduction are manifested on the ECG by a change in the shape and increase in the size of the P wave, and with intraventricular block - an increase in QRS. Atrioventricular block can be characterized by the loss of individual complexes, an increase in the P-Q interval, and in the most severe cases, a complete absence of connection between QRS and P.
Important:sinoatrial block appears on the ECG as a rather bright picture; it is characterized by the complete absence of the PQRST complex.
In case of heart rhythm disturbances, electrocardiography data is assessed based on the analysis and comparison of intervals (inter- and intra-cycle) for 10-20 seconds or even longer.

Important diagnostic value when diagnosing arrhythmias, they have the direction and shape of the P wave, as well as the QRS complex.
Myocardial dystrophy
This pathology is visible only in some leads. It is manifested by changes in the T wave. As a rule, its pronounced inversion is observed. In a number of cases, a significant deviation from the normal RST line is recorded. Pronounced dystrophy of the heart muscle is often manifested by a pronounced decrease in the amplitude of the QRS and P waves.
If a patient develops an attack of angina, then the electrocardiogram shows a noticeable decrease (depression) in RST, and in some cases, inversion of T. These changes in the ECG reflect ischemic processes in the intramural and subendocardial layers of the cardiac muscle of the left ventricle. These areas are the most demanding for blood supply.
Note:a short-term rise in the RST segment is characteristic feature pathology known as Prinzmetal's angina.
In approximately 50% of patients, between attacks of angina, changes on the ECG may not be recorded at all. 
In this life-threatening condition, an electrocardiogram provides information about the extent of the lesion, its exact location and depth. In addition, an ECG allows you to monitor the pathological process over time.
Morphologically it is customary to distinguish three zones:
- central (zone of necrotic changes in myocardial tissue);
- the zone of pronounced dystrophy of the heart muscle surrounding the lesion;
- peripheral zone of pronounced ischemic changes.
All changes that are reflected on the ECG change dynamically according to the stage of development of myocardial infarction.

Dishormonal myocardial dystrophy
Myocardial dystrophy, caused by a sharp change in the patient’s hormonal background, is usually manifested by a change in the direction (inversions) of the T wave. Depressive changes in the RST complex are much less common.
Important: The severity of changes may vary over time. Pathological changes recorded on the ECG are only in rare cases associated with such clinical symptoms as pain syndrome in the chest area.
To distinguish the manifestations of coronary artery disease from myocardial dystrophy against the background of hormonal imbalance, cardiologists practice tests using such pharmacological agents, such as β-adrenergic blockers and potassium-containing drugs.
Changes in electrocardiogram parameters while the patient is taking certain medications
Changes in the ECG pattern can be caused by taking the following drugs:
- drugs from the group of diuretics;
- drugs related to cardiac glycosides;
- Amiodarone;
- Quinidine.
In particular, if the patient takes digitalis preparations (glycosides) in recommended doses, then relief of tachycardia (rapid heartbeat) and a decrease in the Q-T interval are determined. “Smoothing” of the RST segment and shortening of T are also possible. An overdose of glycosides is manifested by such serious changes as arrhythmia (ventricular extrasystoles), AV block and even a life-threatening condition - ventricular fibrillation (requires immediate resuscitation measures).
The pathology causes an excessive increase in the load on the right ventricle, and leads to its oxygen starvation and rapidly increasing dystrophic changes. In such situations, the patient is diagnosed with “acute cor pulmonale.” In the presence of pulmonary embolism, blockade of the branches of the His bundle is not uncommon.
The ECG shows a rise in the RST segment in parallel in leads III (sometimes in aVF and V1,2). There is T inversion in leads III, aVF, V1-V3.

Negative dynamics increase rapidly (a matter of minutes pass), and progression is noted within 24 hours. With positive dynamics, the characteristic symptoms gradually disappear within 1-2 weeks.
Early repolarization of the cardiac ventricles
This deviation is characterized by an upward shift of the RST complex from the so-called isolines. Another characteristic sign is the presence of a specific transition wave on the R or S waves. These changes in the electrocardiogram have not yet been associated with any myocardial pathology, therefore they are considered a physiological norm.
Pericarditis
Acute inflammation of the pericardium is manifested by a significant unidirectional elevation of the RST segment in any leads. In some clinical cases, the displacement may be discordant.
Myocarditis
Inflammation of the heart muscle is noticeable on the ECG by deviations from the T wave. They can vary from a decrease in voltage to an inversion. If, in parallel, the cardiologist conducts tests with potassium-containing drugs or β-blockers, then the T wave remains negative.
Decoding an ECG is the job of a knowledgeable doctor. With this method functional diagnostics estimated:
- heart rate - the state of the generators of electrical impulses and the state of the heart system conducting these impulses
- condition of the heart muscle itself (myocardium), the presence or absence of inflammation, damage, thickening, oxygen starvation, electrolyte imbalance
However, modern patients often have access to their medical documents, in particular, to electrocardiography films on which medical reports are written. With their diversity, these records can reach even the most balanced but ignorant person. After all, the patient often does not know for certain how dangerous to life and health is what is written on the back of the ECG film by the hand of a functional diagnostician, and there are still several days before an appointment with a therapist or cardiologist.
To reduce the intensity of passions, we immediately warn readers that with not a single serious diagnosis (myocardial infarction, acute rhythm disturbances), a functional diagnostician will not let a patient leave the office, but, at a minimum, will send him for a consultation with a fellow specialist right there. About the rest of the “open secrets” in this article. In all unclear cases of pathological changes in the ECG, ECG monitoring, 24-hour monitoring (Holter), ECHO cardioscopy (ultrasound of the heart) and stress tests (treadmill, bicycle ergometry) are prescribed.
Numbers and Latin letters in ECG interpretation
PQ- (0.12-0.2 s) – atrioventricular conduction time. Most often it lengthens against the background of AV blockade. Shortened in CLC and WPW syndromes.
P – (0.1s) height 0.25-2.5 mm describes atrial contractions. May indicate their hypertrophy.
QRS – (0.06-0.1s) -ventricular complex
QT – (no more than 0.45 s) lengthens with oxygen starvation (myocardial ischemia, infarction) and the threat of rhythm disturbances.
RR - the distance between the apices of the ventricular complexes reflects the regularity of heart contractions and makes it possible to calculate heart rate.
The interpretation of the ECG in children is presented in Fig. 3
Heart Rate Description Options
Sinus rhythm
This is the most common inscription found on an ECG. And, if nothing else is added and the frequency (HR) is indicated from 60 to 90 beats per minute (for example, HR 68`) - this is the best option, indicating that the heart works like a clock. This is the rhythm set by the sinus node (the main pacemaker that generates electrical impulses that cause the heart to contract). At the same time, sinus rhythm implies well-being, both in the state of this node and the health of the conduction system of the heart. The absence of other records denies pathological changes in the heart muscle and means that the ECG is normal. In addition to sinus rhythm, there may be atrial, atrioventricular or ventricular, indicating that the rhythm is set by cells in these parts of the heart and is considered pathological.
Sinus arrhythmia
This is a normal variant in young people and children. This is a rhythm in which impulses leave the sinus node, but the intervals between heart contractions are different. This may be due to physiological changes (respiratory arrhythmia, when heart contractions slow down during exhalation). Approximately 30% of sinus arrhythmias require observation by a cardiologist, as they are at risk of developing more serious rhythm disturbances. These are arrhythmias after rheumatic fever. Against the background of myocarditis or after it, against the background infectious diseases, heart defects and in persons with a family history of arrhythmias.
Sinus bradycardia
These are rhythmic contractions of the heart with a frequency of less than 50 per minute. In healthy people, bradycardia occurs, for example, during sleep. Bradycardia also often occurs in professional athletes. Pathological bradycardia may indicate sick sinus syndrome. In this case, bradycardia is more pronounced (heart rate from 45 to 35 beats per minute on average) and is observed at any time of the day. When bradycardia causes pauses in heart contractions of up to 3 seconds during the day and about 5 seconds at night, leads to disturbances in the supply of oxygen to tissues and is manifested, for example, by fainting, an operation is indicated to install a cardiac pacemaker, which replaces the sinus node, imposing a normal rhythm of contractions on the heart. 
Sinus tachycardia
Heart rate more than 90 per minute is divided into physiological and pathological. In healthy people, sinus tachycardia is accompanied by physical and emotional stress, drinking coffee, sometimes strong tea or alcohol (especially energy drinks). It is short-lived and after an episode of tachycardia, the heart rate returns to normal within a short period of time after stopping the load. With pathological tachycardia, heartbeats bother the patient at rest. Its causes include fever, infections, blood loss, dehydration, anemia,. The underlying disease is treated. Sinus tachycardia is stopped only in case of a heart attack or acute coronary syndrome.
Extarsystole
These are rhythm disturbances in which foci outside the sinus rhythm give extraordinary cardiac contractions, after which there is a pause of twice the length, called compensatory. In general, the patient perceives heartbeats as uneven, rapid or slow, and sometimes chaotic. The most worrying thing is the dips in heart rate. May occur in the form of tremors, tingling, feelings of fear and emptiness in the stomach.
Not all extrasystoles are dangerous to health. Most of them do not lead to significant circulatory disorders and do not threaten either life or health. They can be functional (against the background panic attacks, cardioneurosis, hormonal imbalances), organic (for ischemic heart disease, heart defects, myocardial dystrophy or cardiopathy, myocarditis). Intoxication and heart surgery can also lead to them. Depending on the place of occurrence, extrasystoles are divided into atrial, ventricular and anthrioventricular (arising in the node at the border between the atria and ventricles).
- Single extrasystoles most often rare (less than 5 per hour). They are usually functional and do not interfere with normal blood flow.
- Paired extrasystoles two each accompany a certain number of normal contractions. Such rhythm disturbances often indicate pathology and require further examination (Holter monitoring).
- Allorhythmias are more complex types of extrasystoles. If every second contraction is an extrasystole, this is bigymenia, if every third contraction is trigymenia, every fourth is quadrigymenia.
It is customary to divide ventricular extrasystoles into five classes (according to Lown). They are assessed during daily ECG monitoring, since the readings of a regular ECG in a few minutes may not show anything.
- Class 1 - single rare extrasystoles with a frequency of up to 60 per hour, emanating from one focus (monotopic)
- 2 – frequent monotopic more than 5 per minute
- 3 – frequent polymorphic (of different shapes) polytopic (from different foci)
- 4a – paired, 4b – group (trigymenia), episodes of paroxysmal tachycardia
- 5 – early extrasystoles
The higher the class, the more serious the violations, although today even grades 3 and 4 do not always require drug treatment. In general, if there are less than 200 ventricular extrasystoles per day, they should be classified as functional and not worry about them. For more frequent cases, ECHO CS is indicated, and sometimes cardiac MRI is indicated. It is not the extrasystole that is treated, but the disease that leads to it.
Paroxysmal tachycardia
In general, a paroxysm is an attack. A paroxysmal increase in rhythm can last from several minutes to several days. In this case, the intervals between heart contractions will be the same, and the rhythm will increase over 100 per minute (on average from 120 to 250). There are supraventricular and ventricular forms of tachycardia. The basis of this pathology is the abnormal circulation of an electrical impulse in the conduction system of the heart. This pathology can be treated. Home remedies to relieve an attack:
- holding your breath
- increased forced cough
- immersing face in cold water
WPW syndrome
Wolff-Parkinson-White syndrome is a type of paroxysmal supraventricular tachycardia. Named after the authors who described it. The appearance of tachycardia is based on the presence of an additional nerve bundle between the atria and ventricles, through which a faster impulse passes than from the main pacemaker.
As a result, an extraordinary contraction of the heart muscle occurs. The syndrome requires conservative or surgical treatment(with ineffectiveness or intolerance of antiarrhythmic tablets, with episodes of atrial fibrillation, with concomitant heart defects).
CLC – syndrome (Clerk-Levi-Christesco)
is similar in mechanism to WPW and is characterized by earlier excitation of the ventricles than normal due to an additional bundle along which the nerve impulse travels. The congenital syndrome is manifested by attacks of rapid heartbeat.
Atrial fibrillation
It can be in the form of an attack or a permanent form. It manifests itself in the form of atrial flutter or fibrillation.
Atrial fibrillation

Atrial fibrillation
When flickering, the heart contracts completely irregularly (the intervals between contractions of very different durations). This is explained by the fact that the rhythm is not set by the sinus node, but by other cells of the atria.
The resulting frequency is from 350 to 700 beats per minute. There is simply no full contraction of the atria; contracting muscle fibers do not effectively fill the ventricles with blood.
As a result, the heart’s output of blood deteriorates and organs and tissues suffer from oxygen starvation. Another name for atrial fibrillation is atrial fibrillation. Not all atrial contractions reach the ventricles of the heart, so the heart rate (and pulse) will be either below normal (bradysystole with a frequency of less than 60), or normal (normosystole from 60 to 90), or above normal (tachysystole more than 90 beats per minute ).
An attack of atrial fibrillation is difficult to miss.
- It usually starts with a strong beat of the heart.
- It develops as a series of absolutely irregular heartbeats with a high or normal frequency.
- The condition is accompanied by weakness, sweating, dizziness.
- The fear of death is very pronounced.
- There may be shortness of breath, general agitation.
- Sometimes observed.
- The attack ends with the normalization of the rhythm and the urge to urinate, in which a large amount of urine leaves.
To stop the attack, they use reflex methods, drugs in the form of tablets or injections, or resort to cardioversion (stimulation of the heart with an electric defibrillator). If an attack of atrial fibrillation is not eliminated within two days, the risks of thrombotic complications (pulmonary embolism, stroke) increase.
With a constant form of heartbeat flicker (when the rhythm is not restored either against the background of drugs or against the background of electrical stimulation of the heart), they become a more familiar companion of patients and are felt only with tachysystole (rapid irregular heartbeats). The main task when detecting signs of tachysystole of a permanent form of atrial fibrillation on the ECG is to slow down the rhythm to normosystole without trying to make it rhythmic.
Examples of recordings on ECG films:
- atrial fibrillation, tachysystolic variant, heart rate 160 b'.
- Atrial fibrillation, normosystolic variant, heart rate 64 b'.
Atrial fibrillation can be developed in the program coronary disease heart, against the background of thyrotoxicosis, organic heart defects, with diabetes mellitus, sick sinus syndrome, intoxication (most often with alcohol).
Atrial flutter
These are frequent (more than 200 per minute) regular contractions of the atria and equally regular, but less frequent contractions of the ventricles. In general, flutter is more common in acute form and is better tolerated than flicker, since circulatory disorders are less pronounced. Fluttering develops when:
- organic heart diseases (cardiomyopathies, heart failure)
- after heart surgery
- against the background of obstructive pulmonary diseases
- in healthy people it almost never occurs
Clinically, flutter is manifested by rapid rhythmic heartbeat and pulse, swelling of the neck veins, shortness of breath, sweating and weakness.
Conduction disorders
Normally, having formed in the sinus node, electrical excitation travels through the conduction system, experiencing a physiological delay of a split second in the atrioventricular node. On its way, the impulse stimulates the atria and ventricles, which pump blood, to contract. If in any part of the conduction system the impulse is delayed longer than the prescribed time, then excitation to the underlying sections will come later, and, therefore, the normal pumping work of the heart muscle will be disrupted. Conduction disorders are called blockades. They may appear as functional disorders, but more often are the results of drug or alcohol intoxication and organic diseases hearts. Depending on the level at which they arise, several types are distinguished.
Sinoatrial blockade
When the exit of an impulse from the sinus node is difficult. In essence, this leads to sick sinus syndrome, slowing of contractions to severe bradycardia, impaired blood supply to the periphery, shortness of breath, weakness, dizziness and loss of consciousness. The second degree of this blockade is called Samoilov-Wenckebach syndrome.
Atrioventricular block (AV block)
This is a delay in excitation in the atrioventricular node of more than the prescribed 0.09 seconds. There are three degrees of this type of blockade. The higher the degree, the less often the ventricles contract, the more severe the circulatory disorders.
- At the first delay allows each atrial contraction to maintain an adequate number of ventricular contractions.
- The second degree leaves part of the atrial contractions without ventricular contractions. It is described in terms of PQ prolongation and ventricular beat prolapse as Mobitz 1, 2, or 3.
- The third degree is also called complete transverse blockade. The atria and ventricles begin to contract without interconnection.
In this case, the ventricles do not stop because they obey the pacemakers from the underlying parts of the heart. If the first degree of blockade may not manifest itself in any way and can be detected only with an ECG, then the second is already characterized by sensations of periodic cardiac arrest, weakness, and fatigue. With complete blockades, brain symptoms are added to the manifestations (dizziness, spots in the eyes). Morgagni-Adams-Stokes attacks may develop (when the ventricles escape from all pacemakers) with loss of consciousness and even convulsions.
Impaired conduction within the ventricles
In the ventricles to muscle cells the electrical signal propagates through such elements of the conduction system as the trunk of the His bundle, its legs (left and right) and branches of the legs. Blockades can occur at any of these levels, which is also reflected in the ECG. In this case, instead of being simultaneously covered by excitation, one of the ventricles is delayed, since the signal to it bypasses the blocked area.
In addition to the place of origin, a distinction is made between complete or incomplete blockade, as well as permanent and non-permanent blockade. The causes of intraventricular blocks are similar to other conduction disorders (ischemic heart disease, myocarditis and endocarditis, cardiomyopathies, heart defects, arterial hypertension, fibrosis, heart tumors). Also affected are the use of antiarthmic drugs, an increase in potassium in the blood plasma, acidosis, and oxygen starvation.
- The most common is blockade of the anterosuperior branch of the left bundle branch (ALBBB).
- In second place is right leg block (RBBB). This blockade is usually not accompanied by heart disease.
- Left bundle branch block more typical for myocardial lesions. In this case, complete blockade (PBBB) is worse than incomplete blockade (LBBB). It sometimes has to be distinguished from WPW syndrome.
- Block of the posteroinferior branch of the left bundle branch may occur in persons with a narrow and elongated or deformed chest. From pathological conditions it is more typical for overload of the right ventricle (with pulmonary embolism or heart defects).
The clinical picture of blockades at the levels of the His bundle is not pronounced. The picture of the underlying cardiac pathology comes first.
- Bailey's syndrome is a two-bundle block (of the right bundle branch and the posterior branch of the left bundle branch).
Myocardial hypertrophy
With chronic overload (pressure, volume), the heart muscle in certain areas begins to thicken, and the chambers of the heart begin to stretch. On the ECG, such changes are usually described as hypertrophy.
- (LVH) – typical for arterial hypertension, cardiomyopathy, a number of heart defects. But even normally, athletes, obese patients and people engaged in heavy physical labor may experience signs of LVH.
- Right ventricular hypertrophy- an undoubted sign of increased pressure in the pulmonary blood flow system. Chronic cor pulmonale, obstructive pulmonary diseases, cardiac defects (pulmonary stenosis, tetralogy of Fallot, ventricular septal defect) lead to RVH.
- Left atrial hypertrophy (LAH)) – with mitral and aortic stenosis or failure, hypertension, cardiomyopathy, after.
- Right atrial hypertrophy (RAH)- at pulmonary heart, tricuspid valve defects, chest deformities, pulmonary pathologies and pulmonary embolism.
- Indirect signs of ventricular hypertrophy- this is a deviation of the electrical axis of the heart (EOC) to the right or left. The left type of EOS is its deviation to the left, that is, LVH, the right type is RVH.
- Systolic overload- This is also evidence of hypertrophy of the heart. Less commonly, this is evidence of ischemia (in the presence of angina pain).
Changes in myocardial contractility and nutrition
Early ventricular repolarization syndrome
Most often, this is a variant of the norm, especially for athletes and people with congenital high body weight. Sometimes associated with myocardial hypertrophy. Refers to the peculiarities of the passage of electrolytes (potassium) through the membranes of cardiocytes and the characteristics of the proteins from which the membranes are built. Considered a risk factor for sudden stop heart, but does not give a clinic and most often remains without consequences.
Moderate or severe diffuse changes in the myocardium
This is evidence of a malnutrition of the myocardium as a result of dystrophy, inflammation () or. Also reversible diffuse changes accompanied by disturbances in water-electrolyte balance (with vomiting or diarrhea), taking medications (diuretics), severe physical exercise.
Nonspecific ST changes
This is a sign of deterioration in myocardial nutrition without severe oxygen starvation, for example, in case of disturbances in the balance of electrolytes or against the background of dyshormonal conditions.
Acute ischemia, ischemic changes, T wave changes, ST depression, low T
This describes reversible changes associated with oxygen starvation myocardium (ischemia). This can be either stable angina or unstable, acute coronary syndrome. In addition to the presence of the changes themselves, their location is also described (for example, subendocardial ischemia). A distinctive feature of such changes is their reversibility. In any case, such changes require comparison of this ECG with old films, and if a heart attack is suspected, troponin rapid tests for myocardial damage or coronary angiography. Depending on the type of coronary heart disease, anti-ischemic treatment is selected.
Advanced heart attack
It is usually described:
- by stages: acute (up to 3 days), acute (up to 3 weeks), subacute (up to 3 months), cicatricial (all life after a heart attack)
- by volume: transmural (large focal), subendocardial (small focal)
- by location of heart attacks: there are anterior and anterior septal, basal, lateral, inferior (posterior diaphragmatic), circular apical, posterobasal and right ventricular.
In any case, a heart attack is a reason for immediate hospitalization.
The whole variety of syndromes and specific changes on the ECG, the difference in indicators for adults and children, the abundance of reasons leading to the same type of ECG changes do not allow a non-specialist to interpret even the finished conclusion of a functional diagnostician. It is much wiser, having the ECG result in hand, to visit a cardiologist in a timely manner and receive competent recommendations for further diagnosis or treatment of your problem, significantly reducing the risks of emergency cardiac conditions.
Cardiovascular diseases are the most common cause of death in post-industrial society. Timely diagnosis and therapy of the cardiovascular system helps reduce the risk of developing heart pathologies among the population.
An electrocardiogram (ECG) is one of the simplest and most informative methods for studying cardiac activity. An ECG records the electrical activity of the heart muscle and displays the information in the form of waves on a paper tape.
ECG results are used in cardiology to diagnose various diseases. It is not recommended to perform heart treatment on your own; it is better to consult a specialist. However, to get a general idea, it is worth knowing what the cardiogram shows.
Indications for an ECG
In clinical practice, there are several indications for electrocardiography:
- severe chest pain;
- constant fainting;
- dyspnea;
- exercise intolerance;
- dizziness;
- heart murmurs.
During a routine examination, an ECG is a mandatory diagnostic method. There may be other indications determined by the attending physician. If you have any other alarming symptoms– consult a doctor immediately to determine the cause.
How to decipher a cardiogram of the heart?
A strict plan for deciphering an ECG consists of analyzing the resulting graph. In practice, only the total vector of the QRS complex is used. The work of the heart muscle is presented in the form of a continuous line with marks and alphanumeric designations. Any person can decipher an ECG with certain training, but only a doctor can make the correct diagnosis. ECG analysis requires knowledge of algebra, geometry and an understanding of letter symbols.
ECG indicators that need to be taken into account when interpreting the results:
- intervals;
- segments;
- teeth.
There are strict indicators of normality on the ECG, and any deviation is already a sign of disturbances in the functioning of the heart muscle. Pathology can only be excluded by a qualified specialist - a cardiologist.
ECG interpretation in adults - the norm in the table
Cardiogram analysis
The ECG records cardiac activity in twelve leads: 6 limb leads (aVR, aVL, aVF, I, II, III) and six chest leads (V1-V6). The P wave reflects the process of excitation and relaxation of the atria. The Q, S waves show the depolarization phase of the interventricular septum. R - wave, indicating depolarization of the lower chambers of the heart, and T-wave - relaxation of the myocardium.
 Electrocardiogram analysis
Electrocardiogram analysis The QRS complex shows the time of ventricular depolarization. The time it takes for an electrical impulse to travel from the SA node to the AV node is measured by the PR interval.
Computers built into most ECG devices are capable of measuring the time it takes for an electrical impulse to travel from the SA node to the ventricles. These measurements can help your doctor evaluate your heart rate and certain types of heart block.
Computer programs can also interpret ECG results. And as artificial intelligence and programming improve, they are often more accurate. However, ECG interpretation has many subtleties, so human factors still remain an important part of the assessment.
There may be abnormalities in the electrocardiogram that do not affect the patient’s quality of life. However, there are standards normal indicators cardiac activity, which are accepted by the international cardiological community.
Based on these standards, a normal electrocardiogram in healthy person as follows:
- RR interval – 0.6-1.2 seconds;
- P-wave – 80 milliseconds;
- PR interval – 120-200 milliseconds;
- PR segment – 50-120 milliseconds;
- QRS complex – 80-100 milliseconds;
- J-wave: absent;
- ST segment – 80-120 milliseconds;
- T-wave – 160 milliseconds;
- ST interval – 320 milliseconds;
- The QT interval is 420 milliseconds or less if the heart rate is sixty beats per minute.
- ind.juice – 17.3.
 Normal ECG
Normal ECG Pathological ECG parameters
The ECG in normal and pathological conditions is significantly different. Therefore, it is necessary to carefully approach the decoding of the heart cardiogram.
QRS complex
Any abnormality in the electrical system of the heart causes a prolongation of the QRS complex. The ventricles have greater muscle mass than the atria, so the QRS complex is significantly longer than the P wave. The duration, amplitude, and morphology of the QRS complex are useful in identifying cardiac arrhythmias, conduction abnormalities, ventricular hypertrophy, myocardial infarction, electrolyte abnormalities, and other disease conditions.
Q, R, T, P, U teeth
Abnormal Q waves occur when an electrical signal passes through damaged heart muscle. They are considered markers of previous myocardial infarction.
R-wave depression is also usually associated with myocardial infarction, but it can also be caused by left bundle branch block, WPW syndrome, or hypertrophy of the lower chambers of the heart muscle.
 Table of ECG indicators is normal
Table of ECG indicators is normal T wave inversion is always considered an abnormal value on the ECG tape. Such a wave may be a sign of coronary ischemia, Wellens' syndrome, hypertrophy of the lower cardiac chambers, or a central nervous system disorder.
A P wave with increased amplitude may indicate hypokalemia and right atrial hypertrophy. Conversely, a P wave with reduced amplitude may indicate hyperkalemia.
U waves are most often observed with hypokalemia, but may also be present with hypercalcemia, thyrotoxicosis, or taking epinephrine, class 1A and 3 antiarrhythmic drugs. They are often found in congenital long QT syndrome and intracranial hemorrhage.
An inverted U wave may indicate pathological changes in the myocardium. Another U-wave can sometimes be seen on ECGs in athletes.
QT, ST, PR intervals
QTc prolongation causes premature action potentials during late phases of depolarization. This increases the risk of developing ventricular arrhythmias or fatal ventricular fibrillation. Higher rates of QTc prolongation are observed in women, older patients, hypertensive patients, and short people.
The most common causes of QT prolongation are hypertension and certain medications. The duration of the interval is calculated using the Bazett formula. With this symptom, the interpretation of the electrocardiogram should be performed taking into account the medical history. This measure is necessary to eliminate hereditary influence.
ST interval depression may indicate ischemia coronary arteries, transmural myocardial infarction or hypokalemia.
 Characteristics of all indicators of electrocardiographic research
Characteristics of all indicators of electrocardiographic research A prolonged PR interval (greater than 200 ms) may indicate first-degree heart block. Prolongation may be associated with hypokalemia, acute rheumatic fever, or Lyme disease. A short PR interval (less than 120 ms) may be associated with Wolff-Parkinson-White syndrome or Lown-Ganong-Levine syndrome. PR segment depression may indicate atrial injury or pericarditis.
Examples of heart rate descriptions and ECG interpretation
Normal sinus rhythm
Sinus rhythm is any heart rhythm in which the excitation of the heart muscle begins from the sinus node. It is characterized by correctly oriented P waves on the ECG. By convention, the term "normal sinus rhythm" includes not only normal P waves, but also all other ECG measurements.
 ECG normal and decoding of all indicators
ECG normal and decoding of all indicators ECG norm in adults:
- heart rate from 55 to 90 beats per minute;
- regular rhythm;
- normal PR interval, QT and QRS complex;
- The QRS complex is positive in almost all leads (I, II, AVF and V3-V6) and negative in aVR.
Sinus bradycardia
A heart rate less than 55 in sinus rhythm is called bradycardia. ECG interpretation in adults should take into account all parameters: sports, smoking, medical history. Because in some cases, bradycardia is a variant of the norm, especially in athletes.
Pathological bradycardia occurs with weak sinus node syndrome and is recorded on the ECG at any time of the day. This condition is accompanied by constant fainting, pallor and hyperhidrosis. In extreme cases, pacemakers are prescribed for malignant bradycardia.
 Sinus bradycardia
Sinus bradycardia Signs of pathological bradycardia:
- heart rate less than 55 beats per minute;
- sinus rhythm;
- P waves are vertical, consistent, and normal in morphology and duration;
- PR interval from 0.12 to 0.20 seconds;
Sinus tachycardia
A regular rhythm with a high heart rate (above 100 beats per minute) is commonly called sinus tachycardia. Note that normal heart rate varies depending on age; for example, in infants, the heart rate may reach 150 beats per minute, which is considered normal.
Advice! At home it can help with severe tachycardia coughing or pressing on eyeballs. These actions stimulate the vagus nerve, which activates the parasympathetic nervous system, causing the heart to beat slower.
 Sinus tachycardia
Sinus tachycardia Signs of pathological tachycardia:
- Heart rate is above one hundred beats per minute;
- sinus rhythm;
- P waves are vertical, consistent and normal in morphology;
- PR interval fluctuates between 0.12-0.20 seconds and shortens with increasing heart rate;
- QRS complex less than 0.12 seconds.
Atrial fibrillation
Atrial fibrillation is an abnormal heart rhythm characterized by rapid and irregular contraction of the atria. Most episodes are asymptomatic. Sometimes an attack is accompanied by the following symptoms: tachycardia, fainting, dizziness, shortness of breath or chest pain. The disease is associated with increased risk development of heart failure, dementia and stroke.
 Atrial fibrillation
Atrial fibrillation Signs of atrial fibrillation:
- Heart rate is unchanged or accelerated;
- P waves are absent;
- electrical activity is chaotic;
- RR intervals are irregular;
- QRS complex less than 0.12 seconds (in rare cases, the QRS complex lengthens).
Important! Despite the above explanations with data decoding, an ECG conclusion should be made only by a qualified specialist - a cardiologist or general doctor. Decoding the electrocardiogram and differential diagnosis requires higher medical education.
How to “read” myocardial infarction on an ECG?
Students starting to study cardiology often have a question: how to learn to read a cardiogram correctly and identify myocardial infarction (MI)? You can “read” a heart attack on a paper tape based on several signs:
- ST segment elevation;
- peaked T wave;
- deep Q wave or lack thereof.
When analyzing electrocardiography results, these indicators are first identified, and then the others are dealt with. Sometimes the most early sign acute myocardial infarction is only a pointed T-wave. In practice, this is quite rare because it appears only 3-28 minutes after the onset of a heart attack.
An electrocardiogram (ECG) is instrumental diagnostic method, which determines pathological processes in the heart by recording cardiac electrical impulses. A graphical representation of the activity of the heart muscles under the influence of electrical impulses allows the cardiologist to timely identify the presence or development of cardiac pathologies.
ECG interpretation indicators help to determine with great certainty:
- Frequency and rhythm of heart contraction;
- Diagnose acute or chronic processes in the heart muscle in a timely manner;
- Disorders of the conduction system of the heart and its independent rhythmic contractions;
- See hypertrophic changes in its departments;
- Identify disorders throughout the body water and electrolyte balance and extracardiac pathologies (cor pulmonale).
The need for an electrocardiographic examination is due to the manifestation of certain symptoms:
- the presence of synchronous or periodic heart murmurs;
- syncope signs (fainting, short-term loss of consciousness);
- attacks of convulsive seizures;
- paroxysmal arrhythmia;
- manifestations of coronary artery disease (ischemia) or infarction conditions;
- the appearance of pain in the heart, shortness of breath, sudden weakness, cyanosis of the skin in patients with cardiac diseases.
ECG examination is used for diagnosis systemic diseases, monitoring patients under anesthesia or before surgery. Before clinical examination of patients who have crossed the 45-year mark.
An ECG examination is mandatory for persons undergoing medical commission(pilots, drivers, machinists, etc.) or associated with hazardous production.
The human body has high electrical conductivity, which allows the potential energy of the heart to be read from its surface. Electrodes connected to various parts of the body help with this. In the process of excitation of the heart muscle by electrical impulses, the voltage difference oscillates between certain lead points, which is recorded by electrodes located on the body - on the chest and limbs.
 A certain movement and amount of tension during systole and diastole (contraction and relaxation) of the heart muscle changes, the tension fluctuates, and this is recorded on a chart paper tape with a curved line - teeth, convexity and concavity. Electrodes placed on the limbs (standard leads) create signals and form the tops of triangular teeth.
A certain movement and amount of tension during systole and diastole (contraction and relaxation) of the heart muscle changes, the tension fluctuates, and this is recorded on a chart paper tape with a curved line - teeth, convexity and concavity. Electrodes placed on the limbs (standard leads) create signals and form the tops of triangular teeth.
Six leads located on the chest display cardiac activity in a horizontal position - from V1 to V6.
On the limbs:
- Lead (I) – displays the voltage level in the intermediate circuit of the electrodes located on the left and right wrist (I=LR+PR).
- (II) – records on the tape the electrical activity in the circuit – ankle of the left leg + wrist of the right hand).
- Lead (III) – characterizes the voltage in the chain of fixed electrodes of the wrist of the left hand and ankle of the left leg (LR + LN).
If necessary, additional leads are installed, reinforced ones - “aVR”, “aVF” and “aVL”.


Interpretation of ECG diagram, photo
The general principles of deciphering a cardiac cardiogram are based on the readings of the elements of the cardiography curve on the chart tape.
The teeth and bumps in the diagram represent in capital letters Latin alphabet – “P”, “Q”, “R”, “S”, “T”
- The convexity (wave or concavity) of the “P” reflects the function of the atria (their excitation), and the entire complex of the upward-pointing wave is the “QRS”, the greatest spread of the impulse through the cardiac ventricles.
- The “T” convexity characterizes the restoration of the potential energy of the myocardium (the middle layer of the heart muscle).
- When deciphering ECGs in adults, special attention is paid to the distance (segment) between adjacent elevations - “P-Q” and “S-T”, which reflect the delay of electrical impulses between the cardiac ventricles and the atrium, and the “TR” segment - relaxation of the heart muscle in the interval (diastole) .
- The intervals on the cardiographic line include both elevations and segments. For example - "P-Q" or "Q-T".
Each element in the graphic image indicates certain processes occurring in the heart. It is by the indicators of these elements (length, height, width), location relative to the isoline, features, according to the various locations of electrodes (leads) on the body that the doctor can identify the affected areas of the myocardium, based on the readings of the dynamic aspects of the energy of the heart muscle.
Interpretation of ECG - the norm in adults, table
The analysis of the ECG decoding result is carried out by assessing the data in a certain sequence:
- Determination of heart rate indicators. With the same interval between the “R” teeth, the indicators correspond to the norm.
- The heart rate is calculated. This is determined simply - the ECG recording time is distributed by the number of cells in the interval between the “R” teeth. With a good cardiogram of the heart, the frequency of contractions of the heart muscle should be within the limits not exceeding 90 beats/min. A healthy heart should have sinus rhythm, it is determined mainly by the elevation of “P”, reflecting the excitation of the atria. By wave motion this indicator norm is 0.25 mV with a duration of 100 ms.
- The norm for the size of the depth of the “Q” wave should not be more than 0.25% of the fluctuations in the elevation of “R” and the width of 30 ms.
- The latitude of oscillations of the “R” elevation, during normal heart function, can be displayed with a large range ranging from 0.5-2.5 mV. And the activation time of excitation above the zone of the right cardiac chamber - V1-V2 is 30 ms. Above the left chamber zone – V5 and V6, it corresponds to 50 ms.
- According to the maximum length of the “S” wave, its normal dimensions at the greatest abduction cannot cross the threshold of 2.5 mV.
- The amplitude of the "T" fluctuations of the elevation, which reflects the restorative cellular processes of the initial potential in the myocardium, should be equal to ⅔ of the fluctuations of the "R" wave. The normal interval (width) of the "T" elevation can vary (100-250) ms.
- The normal ventricular firing complex (QRS) width is 100 ms. It is measured by the interval between the beginning of the “Q” and the end of the “S” teeth. The normal amplitude of the duration of the "R" and "S" waves is determined by the electrical activity of the heart. The maximum duration should be within 2.6 mV.
| ECG decoding for adults norm in the table | |
| Index | Meaning |
| QRS | 0.06-0.1 s |
| P | 0.07-0.11 s |
| Q | 0.03 s |
| T | 0.12-0.28 s |
| P.O. | 0.12-0.2 s |
| Heart rate | 60-80 beats minute |
Interpretation of ECG in children, normal indicators
The electrocardiogram in children, as practice shows, is not much different from the norm in adult patients. But certain physiological age characteristics may change some indicators. In particular, heart rate. In young children under 3 years old, they can range from 100 to 110 contractions/minute. But already at puberty, it is equal to adult indicators (60-90).
Normally, when deciphering the ECG of the heart in children, the passage of electrical impulses through the parts of the heart (in the interval of elevations P, QRS, T) varies 120-200 ms.
The indicator of ventricular excitation (QRS) is determined by the width of the interval between the "Q" and "S" waves and should not cross the boundaries of 60-100 ms.
Particular attention is paid to the size (excitation activity) of the right ventricle (V1-V2). In children this figure is higher than in the left ventricle. With age, the indicators return to normal.
- Quite often on the ECG in babies there are thickenings, splitting or notches on the "R" hills. Such a symptom in the cardiogram of adults indicates tachycardia and bradycardia, and in children it is quite a common condition.
But there are indications of a bad cardiogram hearts that indicate the presence or progression pathological processes in heart. Much depends on the child’s individual performance. In addition, interruption or slowing of the normal heart rate is seen in children with chest pain, dizziness, frequent signs of blood pressure instability or impaired coordination.
If an ECG examination of a child reveals that the heart rate exceeds 110 beats/min. - this is an alarming signal that speaks of the development of tachycardia.
It is necessary to immediately reduce the child’s physical activity and protect him from nervous overexcitation. In children, such symptoms may be temporary, but if measures are not taken, tachycardia will develop into a permanent problem.
Example ECG - Atrial tachycardia



